Edited by Dr. Giovanni Chetta
Diagnosis of scoliosis

Scoliosis is frequently identified by chance due to its aesthetic evidence or by means of instrumental examinations (radiographs, magnetic resonances, etc.) performed for other reasons.
Some signs that can raise the suspicion of a scoliotic presence are:
- Obvious inequality of the two triangles of the size;
- A shoulder considerably superior to the contralateral;
- Obvious tilt (and rotation) of the pelvis;
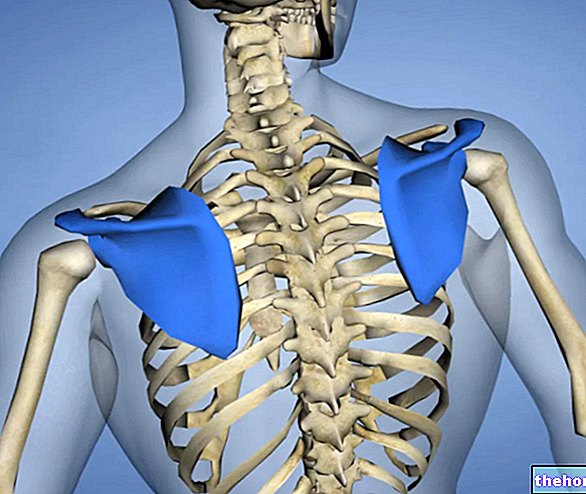
- One shoulder blade much more prominent than the other;
- Obvious inclination of the head and / or the whole body to one side;
- Obvious difference in the right plantar support compared to the left.
During a specialist visit, the subject is usually examined statically and dynamically in three positions: standing (alignment of shoulders, hips, triangles of size, chest, pelvis, shoulder blades, plumb line), anterior flexion or Adams (examination of vertebral alignment and hump using scoliosometer), lying position (verification of the length of the lower limbs, vertebral column and paravertebral musculature).
Head and trunk movements are also performed by evaluating joint mobility and muscle-ligament elasticity.
Unfortunately, too little often tests are also performed on proprioception, in particular on the main articular hinges, and on motor coordination, in my opinion of fundamental importance. It should in fact be emphasized that deformations of the spine such as scoliosis see a preponderant involvement of the deep postural musculature, composed of type I, red, slow twitch (Slow Twitch) and resistant muscle fibers, as they present a slow oxidative process (Slow Oxidative). By its nature and function, this musculature is strongly linked to proprioceptive stimuli. On the basis of their reflex interpretation, these muscles (also defined as phasic) determine, moment by moment, a specific three-dimensional attitude of the myofascial tensegrity network (described below) and therefore, in addition to the spinal curves, the entire posture.
On the basis of all this, an initial diagnosis and hypotheses (which can only be approximate) on the degree of correctability of the scoliotic curve are formulated.
When the visual examination highlights the existence of scoliosis, an in-depth examination is obviously performed through specific instrumental examinations. Among these, the most used to date is the radiographic one performed in standing position and, in some cases, in supine position (bending test or Adams test, lateral bending). The radiographs allow a "structural analysis of the vertebrae, highlighting any defects / deformations, and the calculation of the Cobb angle".
Limits of the Cobb angle, of the radiographies and of the scoliosometer
According to various authors, it is believed to be in the presence of scoliosis when the calculated Cobb angle exceeds 5 °, over 20 ° the brace can be prescribed, over 40-45 ° surgery.
Regarding the Cobb angle, however, it must be borne in mind that it is a graphic measurement, performed on a radiographic plate, two-dimensional and subject to tracing, interpretation and reading errors. The clinical value of the Cobb angle actually results in the first place from the diffusion of this unit of measurement since, from a biomechanical point of view, the Cobb angle is not better than other units of measurement either for predictivity or precision. The measurement of the lateral deviation of the reconstructed spine represents, for example, a valid alternative. In fact, it allows a simpler graphical determination with respect to the Cobb angle: the straight line joining the VII cervical vertebrae and the IV lumbar vertebra is drawn and its length (Y) is determined, the perpendicular distance drawn between Y and the center of the apical vertebrae of the scoliotic curve represents the lateral deviation (X1). In the case of double curve scoliosis, the two lateral deviations (X1 and X2) are measured and the relative lateral deviation = (X1 + X2) / Y .
A relative lateral deviation of 5, determined by radiography, therefore corresponds to approx. 20 ° Cobb. In the transformation from the lateral radiographic deviation to that of the reconstructed spine using the rasterstereographic method (described in the "Clinical case" chapter), an error of 5-6 ° Cobb must be considered. However, this error is relativized during the follow-up, in which it is the reproducibility of the measurement and the identification of a possible increase in the Cobb angle to be decisive. Since the repeatability of the relative rasterstereographic lateral deviation is similar to the radiographic one, this transposition of the results is therefore possible. The measurement of the relative lateral deviation of the reconstructed spine by means of the rasterstereographic method therefore represents a valid alternative in the diagnosis of scoliosis (Hackemberg, 2003).
Furthermore, the Cobb angle is not able to provide a measure of the asymmetry or the aesthetic appearance of the back. for example they are aesthetically less evident than those with a curve as they are more compensated) because they lack the components of asymmetry: lateral deviation and rotation. To quantify the aesthetic defect it would therefore be appropriate to identify the measure of lateral deviation and transverse rotation; parameters these detectable with the rasterstereography.

The clinical relevance of the morphological analysis of the trunk, as an alternative to the radiographic structural one, therefore arises from three important factors:
- The need to avoid subjecting subjects, generally young (and therefore more sensitive), to regular radiological checks with the consequent load of radiation and related oncogenic risk.
- The poor reliability of radiographic investigations in three-dimensional alterations of the spinal column (radiographs do not allow to accurately determine vertebral rotation, a parameter of great clinical importance in the evaluation of spinal deformity).
- The impossibility of objectively evaluating the aesthetic aspect deriving from the morphological defect, a factor that is of great importance for the subject, through radiographs and clinical examination.
The studies therefore confirm the clinical relevance of rasterstereography in the morphological analysis of the trunk in relation to the diagnosis and follow-up of spinal deformations (scoliosis, dorsal hyperkyphosis, lumbar hyperlordosis, etc.) also important as well as in the pre and post operative phase. considering the need to subject subjects generally of young or childhood age to regular radiological checks, with the consequent load of radiation (X-rays) which results in a significant increase in oncogenic risk, despite the poor reliability of radiographic investigations in the three-dimensional morphological deformations of the spine, such as scoliosis Thanks to this innovative system, radiographic investigations on patients have been reduced by over 70% in Germany (Hackemberg, 2003).
The radiographic examination, on the other hand, plays an irreplaceable role in highlighting, as already mentioned, any bone structural defects, especially vertebral ones.
Other articles on "Diagnosis Scoliosis"
- Scoliosis - Causes and Consequences
- Prognosis of scoliosis
- Treatment of scoliosis
- Extra-Cellular Matrix - Structure and Functions
- Connective tissue and Connective fascia
- Connective Band - Features and Functions
- Posture and tensegrity
- Man's motion and the importance of breech support
- Importance of correct breech and occlusal supports
- Idiopathic Scoliosis - Myths to Dispel
- Clinical case of Scoliosis and Therapeutic Protocol
- Treatment Results Clinical Case Scoliosis
- Scoliosis as a natural attitude - Bibliography