What does it mean?
When cholesterol values remain high, despite an appropriate diet and regular exercise, it is referred to as familial hypercholesterolemia or primary hypercholesterolemia.

Cholesterol values: What do they depend on?
We know that total cholesterol derives from both diet and endogenous synthesis; in particular, about 80-90% is produced by our organism - especially by the liver, but also by the adrenal glands and the sex glands - while the remaining portion originates dietetic.
Types of Hereditary Hypercholesterolemia
Doctors prefer to speak of primary hypercholesterolemia on an heredogenic basis, of which three main forms are known:
- the "polygenic hypercholesterolemia,
- l "familial hyperlipidemia (and combined hyperlipidemia)
- l "primary hypercholesterolemia.
Among all, the most widespread (over 2/3 of cases) is polygenic hypercholesterolemia, in which disnutritional and environmental factors add up and aggravate the underlying dysmetabolism on a multi-genetic basis.
Polygenic hypercholesterolemia is particularly widespread among Westerners, where it affects up to 20% of the population.
On the other hand, the monogenic form, called essential or primitive familial hypercholosterolemia, is rarer, affecting one in 500 heterozygous individuals and one in 1 million homozygous individuals. In this case the disease is caused by an "insufficient activity of the LDL receptor, due to an" alteration of the gene that codes for this protein; it follows that the blood levels of LDL increase in proportion to the reduction in receptor activity, ranging from about 50 to 90-95%. The parallel increase in cholesterolemia is due to the high percentage of cholesterol contained within this lipoprotein class (not surprisingly called bad cholesterol).
Typical of familial hypercholesterolemia, but rare in other forms of primary hypercholesterolemia, are the cholesterol deposits (xanthomas, xanthelasms), which appear earlier the more severe the disease. Unfortunately, patients affected by the essential familial form have a " high and early tendency to the development of coronary heart disease and its expressions (angina pectoris and myocardial infarction), which is clearly higher for homozygotes than for heterozygotes.
Finally, familial hyperlipidemia with multiple phenotypes is associated with a more complex lipidemic alteration. Epidemiologically, isolated increases in cholesterol, triglycerides or both are found in similar percentages. The different expression of the lipidemic anomaly can also be observed in the same subject, who in various circumstances can present different dyslipidemias. The incidence in the population is around 2%.
Treatment
As anticipated at the beginning of the article, in the presence of family hypercholesterolemia (in a broad sense) even a well-planned and well-followed diet can fail the goal of reaching an acceptable lipid structure. It is however important to intervene in the first instance on nutrition, possibly associating it to regular physical exercise (after consulting a doctor). Dietary recommendations are generally based on these points:
- reduce the total energy intake in overweight subjects
- reduce total dietary fat to less than 30% of total energy
- reduce the intake of saturated fatty acids (food of animal origin) to less than 10% of the total energy
- reduce, possibly eliminate, foods rich in hydrogenated oils (present in margarine and in many baked goods)
- reduce the consumption of carbohydrates with a high glycemic index (particularly sweet foods, such as pastry and some types of fruit)
- encourage the consumption of oleic acid (present in olive oil) and linoleic acid (present in fish)
- encourage the use of complex carbohydrates
- increase the consumption of fruit (except bananas, figs, grapes, persimmons and dehydrated fruit), vegetables and legumes
- moderate the salt intake.
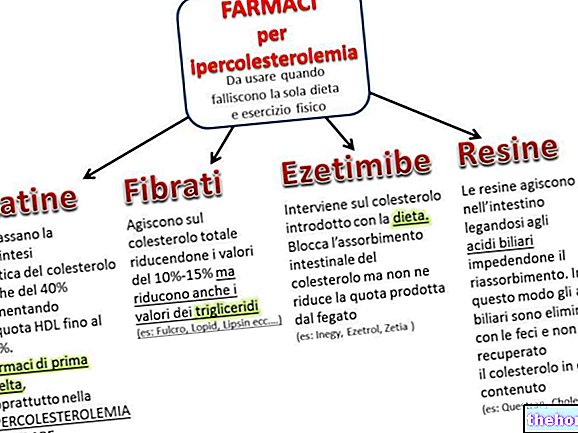
Any failure of the diet requires the use of lipid-lowering drugs, which, however, must not be substituted, but associated with it, in order to exploit the synergistic action of the two therapeutic interventions. The most commonly used drugs in the presence of familial hypercholesterolemia are statins (inhibitors of HMG-CoA reductase) and fibrates (more useful in the presence of high triglycerides). Other drugs commonly used are ezetimibe, niacin and acid sequestrants. biliary.