Causes and classification
None of the symptoms described in the introductory article are specific to a particular type of glomerulonephritis; a kidney biopsy is required for a diagnosis of certainty.
Very often glomerulonephritis recognize an autoimmune genesis, frequently induced by an infectious disease. The etiological mechanisms are complex and not yet fully understood; the key element of the pathogenetic process has however been identified in the abnormal or excessive response of the antibody system, capable of causing lesions to the components of the renal glomerulus in a direct or indirect manner.
The following presupposes a thorough understanding of the anatomy and physiology of the renal glomerulus.
Primary glomerulonephritis with prevalent nephritic syndrome are:
- Acute post-infectious glomerulonephritis: caused by group A B-haemolytic streptococci or other bacterial or protozoal agents. Generally it starts with a fairly acute clinical picture
- Rapidly progressive glomerulonephritis (GNRP): characterized by a rapid and progressive increase in plasma creatinine values, an expression of a rapid (a few days) deterioration of renal function. Depending on the etiology, it is divided into three subgroups:
- GNRP with anti-basement membrane antibodies
- GNRP from immune complexes
- GNRP pauci-immune
- Glomerulonephritis with IgA mesangial deposits (Berger's disease or disease): it is the most frequent form of primary glomerulonephritis, often characterized by arterial hypertension and pathological changes in the urinary level. Mesangial deposits of IgA are appreciated at the glomerular level, in the absence of systemic, hepatic diseases or affections of the lower urinary tract. About 30% of patients develop "end-stage renal failure" over the years
It often occurs as a consequence of systemic diseases, such as SLE, Schonlein-Henoch purpura, Goodpasture's syndrome. Prompt diagnosis and immediate treatment are needed to avert the bad outcome.
Primary glomerulonephritis with prevalent nephrotic syndrome are:
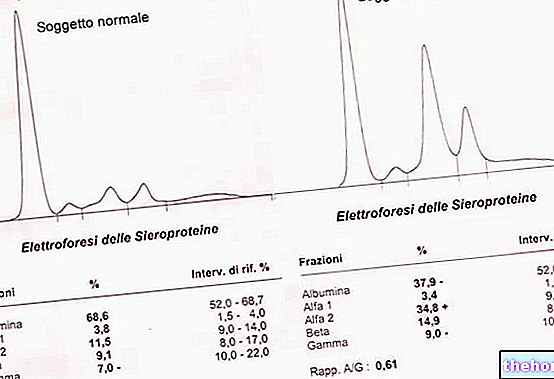
- Glomerulonephritis with minimal lesions: gives rise to significant losses of albumin; glomerular alterations are minimal, detectable only by electron microscopy, and such as to compromise the permeability but not the filtering capacity
- Focal or segmental glomerulonephritis: the term "focal" derives from the limited number of glomeruli affected by sclerotic lesions, which typically affect the glomeruli of the juxtamedullary area of the renal cortex; more frequent in children than in adults
- Membranous glomerulonephritis: it is triggered by immune complexes, often characterized - in addition to the nephrotic syndrome - by a deposition of protein material on the epithelial side of the basement membrane, which causes a thickening of the wall of the fenestrated glomerular capillaries, with the formation of extroflexions of the basement membrane (spikes ) that insinuate themselves between the deposits under the epithelial cells
- Membrano-proliferative glomerulonephritis (mesangio-capillary): characterized by "thickening of the basement membrane due to the proliferation of mesangial cells.The disease often begins before thirty "years of age and usually has a slow and progressive course; unfortunately, late diagnosis does not help treatment: if it is discovered when hypertension and renal insufficiency are already present, the prognosis is poor.
Let's now look at some examples of the many causes responsible for the different forms of glomerulonephritis.
Infectious processes
- Post-streptococcal glomerulonephritis: in the past the classic course of glomerulonephritis was described as a sudden onset of edema, arterial hypertension and changes in the urinary picture, about 10-14 days after a "streptococcal infection of the upper respiratory tract. Currently, we know that post-streptococcal glomerulo-nephritis are only one of the possible forms of presentation.
As anticipated, post-streptococcal glomerulonephritis can develop within a week or two of a "streptococcal throat infection or, rarely, a" skin infection (erispela, impetigo). The etiological agent is group A hemolytic streptococcus (Streptococcus pyogenes). The excessive production of antibodies to the bacterium can cause some of these to travel to the kidney glomeruli, attacking them (immune-mediated damage). Symptoms of post-streptococcal glomerulonephritis include swelling, oliguria (reduced urinary excretion) and hematuria. the disease prefers the male sex (M / F ratio of 2/1) and mainly affects children between 3 and 10 years of age, who in any case - compared to adults - have greater capacity for rapid and spontaneous healing. In industrialized countries, the " health care ensures complete recovery for the vast majority of pediatric patients (mortality rate below 1%), while in the immunocompromised and debilitated elderly the mortality rate can reach 20%. In some patients there is the onset of chronic glomerulonephritis : even if the patients are apparently healthy, the urinalysis shows signs of hematuria, proteinuria and cylindruria, and unfortunately with Over the years, renal function can progressively deteriorate up to uremia. - Bacterial endocarditis: In some circumstances, bacteria can invade the bloodstream and from there be pushed to the heart, where they cause heart valve infections known as endocarditis. Data in hand, there is a frequent association between endocarditis and glomerulonephritis, although this relationship is not yet clear from the pathophysiological point of view.
- Viral infections: some diseases caused by viruses, first of all AIDS and type B and C hepatitis, can favor the onset of glomerulonephritis
- Among the high etiological agents implicated in the onset of acute endocarditis, we recall pneumococcus, varicella viruses, malaria parasites and coxachias.
Autoimmune Diseases
- SLE (systemic lupus erythematosus): it is a chronic inflammatory disease on an autoimmune basis, in which the inflammatory process can extend to various body sites, such as the skin, joints, blood cells, heart, lungs and precisely the kidneys.
- Goodpasture syndrome: rare immunological pulmonary disease that from a clinical point of view manifests itself in a manner similar to pneumonia; Goodpasture's syndrome causes pulmonary haemorrhages and glomerulonephritis
- Glomerulonephritis with IgA mesangial deposits. Autoimmune disease characterized by recurrent episodes of hematuria; by directly targeting the kidney with IgA antibodies, it is the most frequent cause of glomerulonephritis. Its progression can be very slow and asymptomatic, but inexorable: about 30% of patients develop over the years a "terminal renal failure.
Vasculitis
- Polyarteritis: This form of vasculitis affects the small and medium-sized blood vessels that supply various organs of the body, such as the heart, kidneys and intestines.
- Wegner's granulomatosis: This form of vasculitis affects the small to medium-sized blood vessels of the lungs, upper airways, and kidneys.
Conditions that can promote healing of the glomeruli
- Hypertension: as we have seen, high blood pressure can be both a consequence of the kidney damage associated with glomerulonephritis and a predisposing factor for its origin.
- Diabetic nephropathy: complication that afflicts 30-40% of people with type 1 diabetes and 10-20% of type 2 diabetics. Although in a very slow and progressive way, passing through an initial phase of compensation, the disease deteriorates kidney function slowly beyond recovery.
Therapy
The choice of therapy obviously depends on the pathology of which glomerulonephritis is a consequence and expression. For example, post-streptococcal glomerulonephritis is treated with antibiotics, such as penicillin, amoxicillin and erythromycin; on the other hand, in the case of glomerulonephritis associated with nephrotic syndrome, corticosteroids and immunosuppressive drugs seem to ensure a moderate therapeutic success.
Unfortunately, in some cases, the causes of origin of the renal inflammatory process are not known, so in the absence of a well-established etiological therapy, general rules are adopted:
Acute glomerulonephritis:
- Low-sodium and low-protein diet
- Rest in bed initially
- Possible use of anti-hypertensive drugs
Chronic glomerulonephritis:
- Low protein diet (discussed), indicated if renal insufficiency persists or is particularly severe
- Antihypertensive therapy
- Vitamin D
- EPO
- Statins
- Physical activity indicated
- Possible use of anti-hypertensive drugs