What is Cordocentesis?
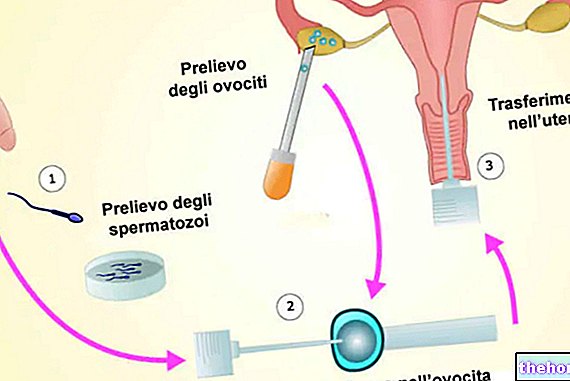
Cordocentesis, better known as funiculocentesis, is an invasive diagnostic procedure, based on the sampling of about 1-3 ml of fetal blood by puncture of the umbilical cord.
Compared to other invasive prenatal techniques, always aimed at taking fetal biological samples (see amniocentesis and chorionic villus sampling), funiculocentesis has a series of limitations that considerably restrict its field of use. In general, however, this examination allows the execution of analyzes useful for prenatal diagnosis, and represents a valuable tool for providing intravascular therapies to the fetus.
How it is done
The examination begins with a preliminary ultrasound check, necessary to ascertain fetal viability, the gestational period and the best access route to the umbilical cord.

Regardless of the route of access, cordocentesis is performed under strict high-resolution ultrasound control, using a 20-22 gauge needle inserted into the uterine cavity by transabdominal route (puncture of the maternal abdomen, previously disinfected, sometimes under local anesthesia).
The puncture, regardless of the site, is preferably performed on the umbilical vein, as the risk of fetal bradycardia associated with removal from the funicular arteries is greater.
At the end of the sampling, the fetus is subjected to a further harmless ultrasound check, in order to ascertain the absence of major haemorrhages at the puncture site, the formation of hematomas or thrombi (very rare) and the fetal heart activity. In non-immunized Rh negative women with Rh positive partners (see Coombs test in pregnancy) it is necessary to undertake a seroprophylaxis with anti-D immunoglobulins, in order to avoid phenomena of maternal-fetal incompatibility.
The greater invasiveness of cordocentesis compared to other methods of direct prenatal diagnosis, recommends its execution in a day-hospital regime; alternatively, the procedure can also be performed on an outpatient basis, provided that complex therapeutic aids are readily available.
* PUBS stands for Percutaneous Umbilical Blood Sample
Indications
When is it performed?
The funiculocentesis is performed after the 18th week of pregnancy, typically between the 20th and 22nd week, the deadline granted by law 194/78 for the voluntary termination of pregnancy (provided that the continuation of gestation represents a serious threat to mental health of the pregnant woman).
The slightly higher abortion rate than other invasive prenatal diagnosis methods limits the use of cordocentesis to cases in which the risk of disease is higher than the risk of abortion associated with the method. In particular, typical indications for cordocentesis are represented by:
- ultrasound suspicion of chromosomal abnormality found with morphological ultrasound of the 20th week;
- need for a rapid assessment of the fetal chromosomal kit (5 - 7 days) to proceed with a "possible termination of pregnancy within the terms permitted by law;
- late use of invasive prenatal diagnosis in patients with specific risks;
- culture failure of the amniocentesis, which on average occurs in 2 cases every 1000 samples (remember that amniocentesis is usually performed between the 15th and 18th week and takes up to three weeks for the laboratory report);
- the presence of true mosaics at the "amniocentesis or chorionic villus sampling (ie presence of cell lines with different chromosomal makeup in the same sample, therefore potentially in the same individual: for example 46, XX / 47, XX +21, which could indicate a trisomy 21 in mosaic, see Down syndrome).
- diagnosis of fetal anemia (including maternal-fetal incompatibility), platelet disorders, hereditary hemoglobinopathies and coagulopathies; through cordocentesis it is also possible to perform transfusions in the uterus and administer drugs and nutrients to underdeveloped fetuses;
- diagnosis of some congenital infections (less valid indication than in the past given the results obtainable with molecular biology techniques on amniotic fluid).
Cordocentesis is a free test if performed for documented genetic risk or maternal age over 35 years.
2) DNA analysis
2) Serological, haematological analyzes, etc. (specific cases)
1) Cytogenetic investigations: 3 days with direct technique; 3 weeks with culture
2) DNA: 2-3 weeks
2) Other analyzes: variable in relation to the type
* The fetal loss observed after cordocentesis is higher than that which occurs after amniocentesis or chorionic villus sampling and is directly related to the experience of the operator.
Risks
Dangers to the Fetus
Normally, cordocentesis does not require the "execution of" local anesthesia and generally does not involve pain for the pregnant woman.
After sampling, an endoamniotic blood drip lasting a few seconds (35-40% of cases) can be observed by ultrasound, without this entailing any risk for the fetus. Similarly, transient bradycardias are observed in 4.3% of cases, without any consequences for the fetus.
No maternal risks associated with the procedure are reported. On the other hand, the interpretation of the risk of fetal death related to cordocentesis is difficult; the statistical data, which show risk percentages around 3%, must in fact be taken with pliers, given that they are affected by abortion not so much linked to the diagnostic procedure itself. , rather than the underlying fetal pathology (in low-risk cases, for example, the incidence of fetal losses is around 2%). In addition to the gestational age (the risk decreases significantly if the funiculocentesis is performed after the 24th week), the risk depends on the degree of experience and skill of the operator, which requires the choice of doctors with proven experience in performing cordocentesis in specific reference centers.