Potentially capable of affecting male fertility (hence the possibility of having children), oligospermia recognizes numerous causes, including varicocele, genital infections, testicular cancer, testicular trauma, smoking, drug use, alcohol abuse, Klinefelter's syndrome, genetic defects affecting the Y chromosome, etc.
To solve the problem of oligospermia, it is essential to treat the triggering causes, detected during the diagnosis.
Brief review of what spermatozoa are
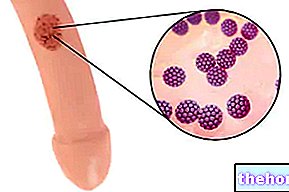
The spermatozoa are the male gametes, that is the cells that, in men, are responsible for the reproductive function, once they meet the female cells with the same task (egg cells).
Produced by the testes (the male gonads) during the so-called spermatogenesis, spermatozoa are very small cellular elements (5-7 micrometers, the diameter, and 70 micrometers maximum, the length) and equipped with a very particular structure, which includes:
- A head, containing the cell nucleus and the acrosome;
- An intermediate portion, rich in mitochondria;
- A tail, endowed with mobility and called a flagellum.
The particular morphology of the spermatozoa is fundamental for the reproductive process, as it allows them to meet and merge with an egg cell, inside the female genital system.
).
Definition of oligospermia according to the WHO
As established by the World Health Organization (WHO) in 2010, a man suffers from oligospermia when, in the sperm produced following a classic ejaculation, the concentration of spermatozoa is less than 15 million per milliliter of sperm (<15 million / ml).
This means that a man capable of producing an ejaculate, in which the concentration of spermatozoa is equal to or greater than 15 million per milliliter, is a man exempt from the oligospermia problem.
Curiously, prior to 2010, the WHO was of a different opinion regarding oligospermia and believed, on the basis of medical knowledge of the time, that a male individual suffered from the aforementioned alteration of semen when, in the ejaculate, the concentration of sperm count was less than 20 million per milliliter.
Table. Reference values that sanction the normality of a human ejaculate, according to the latest indications of the WHO.
Degrees of oligospermia
In addition to specifying in numerical terms when it is possible to speak of oligospermia, the WHO has also defined a scale of severity, as regards the sperm alteration just mentioned.
According to this scale, there are three possible levels (or degrees) of severity of oligospermia: mild, medium and severe.
Oligospermia is mild when the concentration of spermatozoa in the ejaculate is between 10 and 15 million per milliliter (of sperm); it is medium, when the concentration of spermatozoa in the ejaculate is between 5 and 10 million per milliliter; finally, it is severe, when the concentration of spermatozoa in the ejaculate is between 0 and 5 million per milliliter.
Epidemiology
Statistical data relating to the spread of oligospermia in the male population are really scarce. Moreover, conducting a study that evaluates, within a reliable sample, how many men suffer from the aforementioned sperm alteration is not at all simple; in fact, it would require a lot of time, money and the availability of a large number of men (otherwise the statistics are not very reliable).
Origin of the name
The word "oligospermia" derives from the "union of two terms of Greek origin, which are:
- "Oligo" from "oligos"(ὀλίγος), which means" little ", and
- "Spermia" from "semen' (σπέρμα), which means "seed".
Therefore, literally, oligospermia means "little semen" (where by semen s "obviously means the sperm and, specifically, the sperm population).
testicular (or spermatic), as a result of which the latter appear dilated and one or both testicles are swollen. Of the causes of secondary oligospermia, varicocele seems to be the main one; according to some studies, in fact, it is attributable up to 40 % of cases of low sperm concentration in the ejaculate.
- Some infections, such as sexually transmitted infections, malaria and mumps;
- Advanced age. Statistical studies have shown that, as we age, man produces fewer and fewer spermatozoa;
- Hypogonadism. Hypogonadism is the medical term that indicates a more or less marked reduction in the functional activity of the gonads, which in the specific case of man are the testes, followed by a decrease in the production of sex hormones;
- Alcohol abuse, cigarette smoking and the use of drugs, such as hashish, marijuana or cocaine;
- Exposure to toxic agents (eg: chemical solvents, metals, etc.);
- Taking medications, such as beta-blockers, antibiotics, androgens, and high blood pressure medications:
- The presence of a "genital infection, affecting one of those organs in which sperm and seminal fluid usually flow (prostate, seminal vesicles, epididymis and urethra);
- Testicular diseases, such as testicular cancer, hydrocele or cryptorchidism;
- Trauma of a certain extent to damage to the testicles;

- The obstruction of the vas deferens or the ejaculatory ducts. The vas deferens are the small channels that join the epididymis to the seminal vesicles and the ejaculatory ducts; the latter are the small ducts which, crossing the prostate, connect the seminal vesicles to the urethra ;
- The presence of specific genetic defects affecting the sex chromosome Y or genetic diseases, such as Klinefelter syndrome, Noonan syndrome or Kartagener syndrome;
- Obesity. The excess of adipose tissue seems to affect not only the production of spermatozoa, but also the production of sex hormones;
- The habit of behaviors that produce a rise in testicular temperature (eg: repeated practice of saunas, the tendency to wear tight clothing, etc.);
- Benign prostatic hypertrophy, also known as an enlarged prostate or prostate adenoma;
- Chemotherapy and / or radiotherapy, performed on the occasion of a tumor treatment;
- Prolactinoma, a benign tumor of the anterior pituitary gland responsible, in severe cases, for hyperprolactinemia.
Complications
As anticipated, oligospermia can affect a man's fertility and, consequently, the latter's ability to have children.
The "use of" can prejudice "rather than" prejudice "- hence the" idea that "oligospermia does not necessarily mean infertility - is justified by the" observation of men with low concentrations of spermatozoa who managed to have children anyway, without particular problems or at most after several attempts.
Did you know that ...
According to some statistical research, 30-50% of couples wishing to have children, but unable to have them, owe this inability to a problem of male infertility.
Semen abnormalities associated with oligospermia
Not infrequently, oligospermia is accompanied by other alterations of the sperm; among the latter, the asthenozoospermia (reduced number of motile spermatozoa in the sperm) and teratozoospermia (sperm with an abnormal percentage of malformed spermatozoa) deserve a particular mention.
When to see a doctor?
A man with oligospermia should contact a doctor, specifically a urologist or andrologist, when:
- It is his intention to have children, but the alteration of the sperm he suffers from represents an impediment to this intention;
- He has an associated symptom picture that drastically affects his quality of life. In such circumstances, the cause of oligospermia is a clinically relevant condition, which deserves due attention and appropriate treatment.
The spermiogram is a "laboratory investigation, including a first part charged to the patient", which allows you to observe a series of important characteristics of a sperm sample, with the main purpose of establishing the degree of fertility of the "man" owner. "of the aforementioned semen sample.

The characteristics of the sperm, observed by means of a spermiogram, include:
- Sperm viscosity,
- The liquefaction of semen,
- The volume of sperm,
- The number and morphology of spermatozoa e
- The vitality and motility of spermatozoa.
Once the presence of oligospermia has been ascertained, the next step is to search for the causes responsible for the low concentration of spermatozoa in the ejaculate; this research may require the performance of various diagnostic tests, including instrumental tests.
The basic rules for obtaining a reliable spermiogram
In order for the result of a spermiogram to be reliable, it is essential to comply with some preparatory rules for the aforementioned laboratory examination; going into more detail, these preparatory rules are:
- Complete abstinence from sexual activity in the 3-5 days preceding the exam;
- Ejaculation obtained exclusively by masturbation;
- Before masturbation, provide "adequate hand and penis hygiene;"
- Provide for the collection of all the sperm produced (therefore including the one for which it is necessary to press the penis, after the main emissions);
- Collect in a clean place;
- For collection, use a suitable and sterile container (eg urine containers);
- Hermetically close the used container, in such a way as to avoid accidental loss of the sperm sample collected;
- After sample collection, deliver the semen sample to the testing laboratory as soon as possible (within 30-60 minutes), avoiding thermal shock. To simplify everything is the possibility, now increasingly common, to carry out the collection of the sperm sample directly in a bathroom in the analysis laboratory;
- Inform the health personnel of the analysis laboratory of any therapies or illnesses followed or occurred in the last three months;
- Inform the health personnel of the analysis laboratory of any failure to comply with one of the aforementioned preparatory rules, in order to understand whether or not it is necessary to repeat the sperm sample collection procedure.
Tests for the causes of oligospermia
The search for what causes oligospermia always starts from the "physical examination and from the anamnesis; therefore, also on the basis of what emerged from these two tests just mentioned, it can continue with: a blood and urine test, a spermioculture, a "ultrasound of the testicles, one" ultrasound of the lower abdomen, etc.
and balancedAccording to several experts, it would be beneficial for men with oligospermia - as it would improve the quality of spermatogenesis - a healthy and balanced diet, which gives ample space to the consumption of fruit and vegetables (both sources of antioxidants) and to that of foods rich in omega-3 (ex: fish).
Did you know that ...
For men with oligospermia, the chances of having children increase if: they have a "more intense sexual activity, monitor the partner's ovulation to know when" is the time of greatest fertility and, finally, avoid the use of lubricants (reduce mobility of spermatozoa).
When oligospermia persists, but there is a desire for paternity: ICSI
For some time now, men eager to have children but unable to have any because they are affected by oligospermia (or other sperm abnormalities) can rely on a particular technique of assisted reproduction in vitro, known as ICSI or intracytoplasmic injection.

Without going into too much detail, ICSI provides for the specific collection, from a sample of ejaculate, of healthy spermatozoa (therefore well formed, mobile, etc.), the selection of one of these and its inoculation, in vitro, in a cell egg.
Currently, ICSI is one of the most effective non-conventional in vitro fertilization techniques, which can be exploited by men with problems of oligospermia, asthenozoospermia, etc. and who are eager for paternity.