The recognized causes of epiphora are at least three:

- the occlusion (or narrowing) of the system that drains the tears into the nose;
- an "overproduction of tears due to" eye irritation, for example
- an "infrequent (or impossible) blink.
Other signs or symptoms can often be added to the epiphora; these vary according to the favoring causes.
In the presence of epiphora, it is very important to establish the precise reasons for its onset, as this allows to plan the most appropriate treatment.
In less severe cases, the patient may even recover spontaneously; in the most serious situations, however, it requires specific care.
HOW DOES EYE TEAR WORK?
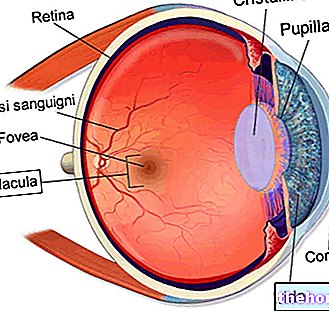
To understand the possible causes of epiphora, it is necessary to briefly describe how ocular tearing occurs and which anatomical structures of the eye are involved in this process.
On the inner face of the upper eyelids, the lacrimal glands reside, which, as you can guess from the name, secrete tears. The activity of the lacrimal glands is constant.
Under normal conditions, tears form a kind of slightly oily liquid film (the so-called tear film), which serves to defend, lubricate, nourish and keep the eye clean.
The volume of tears making up the tear film remains stable, as there is a drainage system on the inner side of the eye which continuously drains excess tears.
The tear discharge system consists of:
- The canaliculi, which are small canals.
- The lacrimal sac, which is a kind of small reservoir fed by the canaliculi.
- The lacrimal duct (or nasolacrimal duct), which is the outlet channel of the lacrimal sac. Through the tear duct, tears are carried into the nose (nasal turbinates) and then into the throat.
When the tear glands are very active or when the drainage system is not functioning properly, excess tears flow from the eyes and copiously wet the cheeks.

EPIDEMIOLOGY
Epiphora is very common among very young children (infants less than one year old) and people over sixty, but, in reality, it can occur in people of any age.
Depending on the underlying cause, it can affect only one eye or both eyes.
The occlusion of the nasolacrimal ducts can be the result of:
- The advanced age
- An "eye inflammation (uveitis or scleritis)
- An eye trauma
- A compression from the outside of the tear ducts
- L "ectropion (ie the condition in which the eyelid faces outward)
When the occlusion affects the canaliculi
Sometimes, in adults, the occlusion of the tear drainage system resides in the canaliculi. Some viral infections or trauma can occlude or narrow the canaliculi.
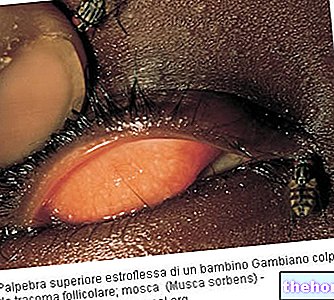
OCCLUSION OF THE TEAR DISCHARGE SYSTEM IN INFANTS (CONGENITAL DACRIOSTENOSIS)
The occlusion of the tear duct (s) in newborns is the result of a delayed development of the tear ducts. Often, after one year of birth, babies with this abnormality recover because the system that drains the tears stops developing.
It is very rare that the occlusion persists after 12 months, but if it does, there is a specific treatment for the release of the tear ducts.
HYPERPRODUCTION OF TEARS BY THE TEAR GLANDS
Excessive tear production by the tear glands can occur for several reasons, such as:
- An "eye irritation. They can irritate the eyes: smoke, dust, some substances released from food (onions, etc.), a conjunctivitis (ie an" eye infection that inflames the conjunctiva), an "allergy, an ocular trauma (due to example to the entry of a grain of sand into the eye), entropion (ie the rotation of the eyelid inwards) and ectropion.
- An abnormal composition of the tear film. The tear film contains various substances: water, mucus, proteins, lipids, etc. If the normal composition of the tear film undergoes a change (for example the lipid content varies), the distribution of the same film on the eye is no longer homogeneous and correct. This triggers an overproduction of tears by the lacrimal glands, tears which then come out of the eye.In fact, it is a compensation mechanism: the tear film is inadequate and the tear glands are activated to remedy this inadequacy.
One of the causes that induces a change in the composition of the tear film is the so-called dry eye syndrome. - Blepharitis. Blepharitis is a "chronic inflammation of the eyelids, which affects the so-called eyelid margin and can cause (precisely on the eyelid margin) redness, swelling, itching, crusts, stinging pain, etc.
Often, the effects of the inflammation just mentioned alter the distribution of the tear film and this causes the tear glands to activate, to bring the tear film back to normal.
It is important to point out that, under the aforementioned circumstances, the tear discharge system works adequately, but the tear production is so massive that its drainage capacity is insufficient. Hence, the tears come out of the eyes.
INFREQUENT OR IMPOSSIBLE BEAT OF THE EYELIDS
Blinking properly is a "key action to direct excess tears to the tear discharge system.
This explains why those who cannot blink, due to some morbid condition (for example Bell's palsy), are also prone to tearful eyes.
The symptoms that can accompany the tearful eye obviously depend on what triggers this ocular condition. For example:
- In case of conjunctivitis, the epiphora are usually added: red eye, burning in the eyes, eye pain, eyelid swelling, itching and / or dry eyes.
- In the case of dry eye syndrome, the following are commonly added to the epiphora: eye fatigue, burning eyes, eye pain, photophobia (ie sensitivity to light), red eyes, itching, dry eye and / or blurred vision.
- In the case of entropion, the epiphora usually adds: eye redness, pain around the eye, photophobia, sensitivity to the wind, relaxation of the skin surrounding the eyes and / or reduced vision.
- In case of an occlusion of the nasolacrimal duct, the epiphora can be joined by: bacterial proliferation in the lacrimal sac, mucocele and / or abscess in correspondence of the mucocele.
WHEN TO SEE THE DOCTOR?
If you suffer from persistent epiphora and other ailments such as eyelid swelling, eye redness etc., it is good to contact your doctor and schedule a check-up.

OPHTHALMOLOGICAL VISIT
During the ophthalmological examination, the ophthalmologist instills anesthetic eye drops into the patient's eye, since the examination involves rather invasive and annoying diagnostic procedures.
Therefore, once anesthesia is performed, he can:
- Inject, through a cannula previously inserted in a lacrimal canaliculus, a sterile solution. If the drainage system is patent, the sterile solution reaches the throat (and the patient senses its presence); if, on the other hand, the draining system is occluded or restricted, the sterile solution remains blocked in a point of the nasolacrimal ducts (and the patient does not feel anything).
- Instill a special contrast liquid in the eyes and evaluate, 5 minutes after application, if and how much this contrast liquid has been drained from the tear discharge system. In the presence of an occlusion or narrowing, after 5 minutes the contrast fluid will still be present on the ocular surface.
- Instill in the eyes a contrast liquid visible to X-rays and observe, using a special instrument for reading ionizing radiation, how this special liquid is distributed inside the tear discharge system. If there is an occlusion, this is perfectly visible on X-rays, as it appears as an "interruption in the passage of the contrast fluid.

If the tear discharge defect is mild and bearable, the patient may try to live with the problem and not resort to special treatments.
If, on the other hand, the occlusion is serious and prevents driving, reading, playing sports or other normal daily activities, it is essential to resort to a special surgical operation, called dacryocystorhinostomy.
Through the operation of dacryocystorhinostomy, the surgeon creates a new nasolacrimal duct thus restoring the drainage (N.B: it is a sort of bypass that eludes the obstacle). The dacryocystorhinostomy requires general anesthesia, lasts about one hour and involves the removal of a small bony plate, located between the eye socket and the nostril.
Finally, remember that, if the stagnation of tears leads to the formation of an abscess, it is necessary to take antibiotics.
Liberation of occluded canaliculi
If the occlusion or narrowing resides in the canaliculi, it is possible to free them by inserting thin glass tubes (in English, these tubes are called Lester Jones Tubes).
HOW TO TREAT THE OCCLUSION OF NOSULACRIMAL DUCTS IN CHILDREN
In most cases, epiphora in infants heals spontaneously once the (still immature) tear discharge system has finished developing. The predicted age for healing is around one year of life.
In the rare cases in which the drainage system remains incomplete (one case out of 10), it is necessary to resort to a specific surgery to reopen the nasolacrimal ducts; this surgery requires general anesthesia.
How to promote tear drainage in infants with immature tear ducts
To promote tear drainage, doctors advise parents to gently massage the inner corner of their baby's eyes. According to some experts, this maneuver would also seem effective in speeding up the maturation of the tear discharge system.
Before performing the massage, it is advisable to always wash your hands very well.