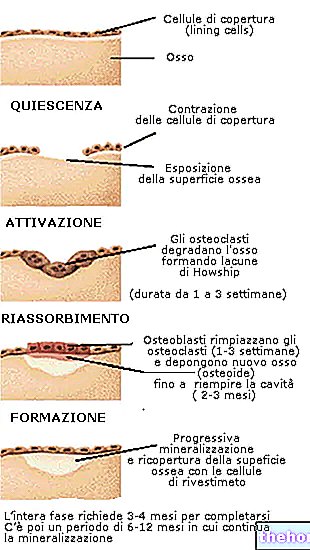
In addition to T3 and T4, the thyroid, with its "parafollicular" or "C cells" (located on the contour of the follicles), produces a third and very important hormone, called calcitonin. Its action is defined as hypocalcemizing, as it is produced and secreted with the aim of lowering calcium in the circulation, hindering its absorption in the intestine, favoring its deposition in the bones and excretion in the kidney. Calcitonin has diametrically opposite activity to that of the parathyroid hormone or parathyroid hormone.
Hormones and Thyroid - Reference Values Blood Analysis
By evaluating, through the simple examination of a blood sample, the plasma concentration of thyroid hormones and TSH it is possible to investigate the activity of the thyroid. When this gland is functioning too much (hyperthyroidism), high levels of T3 and T4 are recorded, but low concentrations of TSH The reverse occurs in the case of reduced production of thyroid hormones (hypothyroidism).
The TRH test is performed by injecting the hormone of the same name into a vein, and then evaluating at set times (0 ", 30", 60 ") the response of the pituitary gland through the TSH dosage; this allows to understand if the reduction in values of the patient's TSH is attributable to the excessive production of thyroid hormones or if there are other abnormalities.
REFERENCE VALUES
Free T3 (FT3): 3.8 - 9.2 pmol / l (2.5-6 pg / ml)
Free T4 (FT4): 10.4 - 26 pml / l (8 - 22 pg / ml)
TG (thyroglobulin): 5-10 ng / mlThe values change in case of: diet too rich or low in iodine (also consider the role of herbal products and supplements); thyroid disease; therapy with thyroid hormones or their inhibitors; radiographic analysis with iodine-containing contrast media.
CT (calcitonin): 8-20 pg / ml.
A sharp increase in these values is recorded in medullary thyroid cancer.
TSH: infants: up to 20 mU / l
basal: 0.1 - 3.5 mU / lElevated TSH levels are generally accompanied by goiter, due to over-stimulation of the thyroid gland.
TRH test: TSH measured 30 minutes after TRH administration: 100 - 200 microUnits / ml.
In the case of hypothyroidism, this peak is significantly higher, while in the presence of hyperthyroidism no TSH peak is observed.
OTHER TESTS: normal oxygen consumption at rest = 250 ml / min,
In case of hypothyroidism this value is lowered to 150 ml / min.
In case of hyperthyroidism it rises up to 400 ml / min
Diseases of the thyroid gland
Hyperthyroidism is defined as a clinical condition characterized by an increase in circulating thyroid hormones.On the other hand, hypothyroidism follows the opposite condition (clinical syndrome characterized by insufficient synthesis or lack of action of T3 and T4 at the tissue level).
Hyperthyroidism can be primary, that is due to thyroid, secondary and tertiary diseases; the former depend on pathologies that increase their activity, such as Graves 'disease or Graves' disease (of autoimmune origin), hyperfunctioning adenoma etc; secondary hyperthyroidisms depend on TSH hyperincretion, usually due to a pituitary tumor; finally, the tertiary forms are caused by excessive hypothalamic secretion of TRH. Whatever its nature, hyperthyroidism causes an increase in oxygen consumption, which results in an increase in cardiac activity, heat production, catabolism and nervous system irritability.
Similar to excess, a defect in the quantity of thyroid hormones (hypothyroidism) can also have primary or secondary origins. Primary hypothyroidisms depend on alterations of the thyroid gland that lower its activity, such as idiopathic atrophy, iodine deficiency in the diet or thyroidectomy ( surgical removal of the thyroid). Secondary hypothyroidisms are related to a deficit in the increase of the two main hormones that regulate the activity of the gland (TRH and TSH) for hypothalamic and / or pituitary pathologies, such as neoplasms, or for their surgical removal.
The symptoms of hypothyroidism depend on the general slowing down of metabolism and nervous function, which causes cretinism in the fetus, reduced statural growth and sexual development in puberty, myxedema in adults (pallor, hoarse voice, myxedematous skin, etc.). Whatever its cause, the faulty synthesis of thyroid hormones stimulates the increase of the thyroid stimulating hormone and its hypothalamic releasing factor. As previously described, the target of these hormones is the thyroid, which accelerates its activity by increasing, like the muscles in response to training, its volume (thyroid hypertrophy or goiter) until it reaches a weight of hundreds of grams.
If this compensation is sufficient, normal thyroid function is maintained (simple goiter), otherwise hypothyroidism with goiter occurs.
In the adult, therefore, thyroid hormones are not essential for survival, but they are important for the quality of life.
Thyroid disorders are quite frequent, affecting an average of one in twenty people, with a clear prevalence in the female population. As mentioned, these dysfunctions can be of various nature (hyperthyroidism, hypothyroidism, abnormal growth of the thyroid gland and, more rarely, tumors of the thyroid gland). Treatment of the disorder, through specific drugs, generally leads to healing and even thyroid cancer, if caught in time, can be eradicated.
PLEASE NOTE: the mere presence of the goiter is not sufficient to establish which pathology afflicts the patient; the increase in volume of the thyroid is in fact a common symptom both in cases of hyper, normal and hypothyroidism.
Diseases of the Thyroid
Problems with playing the video? Reload the video from youtube.
- Go to the Video Page
- Go to Wellness Destination
- Watch the video on youtube
Other articles on "Thyroid Diseases"
- Thyroid
- Thyroid hormones
- Actions of thyroid hormones: thyroxine and triiodothyronine
- Thyroid hormones T3 - T4 and exercise
- Gozzigeni foods
- Hypothyroidism
- Hyperthyroidism
- Triacana