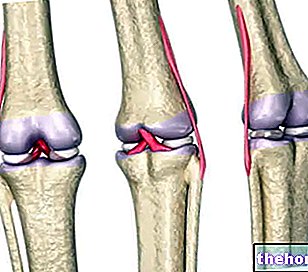
The knee is one of the joints most affected by the functional overload of this activity and, as it is logical to deduce, it is also an often painful area.

In this article we will discuss in more detail patellofemoral pain and new prevention-treatment strategies, highlighting the role of what we could define as the two factors most often responsible: the anterior cruciate ligament and quadriceps femoral weakness.
For reasons of time and space, we will not cover the joint structure of the knee - fully explained in other articles such as this: Knee Pain - as well as the description of the game of volleyball.
In fact, everyone knows that the main component of this discipline is jumping. Most of the time, both in matches and in training, the expression of this gesture is explosive, in itself risky for the integrity of the various structures, both acute and chronic.
However, there are other risk factors or other predisposing factors, such as female sex. Let's find out why.
jump (SJ)Obviously, with variable loads and movements adapted according to the exercise performed and the subjective biomechanics. In reality, however, this expedient is adopted only by a few truly avant-garde centers and with extremely trained technicians. This is obviously a general risk factor, for both young and old, male or female.
However, girls are at a higher risk than boys; in the next paragraph we will find out better why.
and endogenous "T" (testosterone) serum, 0.6 ng / mL for women and 4.6-8.0 ng / mL for men, respectively.
In fact, with the same performance in jumping height, women need more pre-stretching (with eccentric contraction of the quadriceps) than men to equal male performance.
In addition to all this, squat or plyometric exercises with very closed knee angle (<45 °) used in periods of construction or strength recall, require the recruitment of a very large number of Motor Units (MUs) for lifting. of the center of gravity, caused by the fact that at this angle the acto-myosin bridges work in an extremely unfavorable mechanical position for the production of force.
All this can lead to greater wear of the articular fibrocartilages and to an insertional tendinopathy of the quadriceps, as well as to a stress of the anterior cruciate ligament.
In jumping and landing, the major neuromuscular recruitment occurs by the quadriceps, in particular with strong pressure on the anterior cruciate ligament, while in humans it is the hamstrings with stress on the posterior cruciate ligament that offer more valid support to the movement of the jump. and landing.
The myogenic component that controls the knee angle in the upward thrust and downward resistance movement to the ground is prioritized.
In this regard, from the study of biomechanics we know that movement is characterized by
force x (angular velocity + joint angle)
therefore a non-physiological modification of even one of these three parameters will create a deficit in the other two; for example, a decrease in strength in the quadriceps caused by incorrect posture, hypertonicity of the antagonists, excessive fatigue, hormonal imbalances, etc.
The muscular balance of the forces involved, specifically between the vastus medialis and the vastus laterals, is a critical and decisive factor for the onset of joint stress in the patella.
Assuming that the innervation of the quadriceps muscle is always the same (Femoral nerve L2-L3-L4), however, we note that the myogenic activation of the vastus medialis and the vastus lateralis varies in relation to the joint angle of the knee.
The posterior balance between the hamstrings muscles (leg flexors) is also decisive in this problem.
Similarly, sartorius, gracilis, popliteal, tensor fascia lata, and gluteus maximus must be examined in this discussion.
To better understand it is necessary to use a differential diagnosis.
- Sartorius and quadriceps have a common innervation: Femoral nerve L2-L3-L4
- TFL: L4-L5-S1 superior gluteus nerve
- Popliteal: Tibial nerve L4-L5-S1-S2-S3
- Gracilis: Obturator nerve L2-L3-L4
- Hamstrings: Sciatic nerve L4-L5-S1-S2-S3
- Gluteus maximus: L5-S1-S2 inferior gluteus nerve.
In relation to patellofemoral pain and quadriceps weakness with stress of the anterior cruciate ligament in women, these are the identified insults:
- ascending breech dysfunctions
- pelvic category 2 kinesiology
- osteopathic ileosacral torsion
- adrenal stress associated with posterior ileus **
- dysfunctions of the ATM
- deficiency of Ca ++ and Vit.D
- kinesiological subluxation or osteopathic lesion of the pubic symphysis, also associated with posterior ileus *
- cranial and MRP (Primary Respiratory Mechanism) lesions
- intestinal malabsorption, in particular stress of the duodenum, jejunum, ileus
- melancholy, apathy, big emotional disappointments
- amenorrhea, dysmenorrhea ***
* if in association with urgent polyuria, dysuria, discomfort in the area also associated with diastasis from delivery, it is necessary to normalize the pubic symphysis with appropriate maneuvers.
** caused by excess and abuse of carbonated drinks, coffee, refined sugar, carbohydrates, sweets, as well as Basedovian super-training and its complications.
All this leads to stress on the adrenal glands and hypoadrenia.
*** linked to strong emotional tensions, visceral-vertebral disorders or fat mass <17%.
or not, it would be too simple and superficial to stop at the symptom, in this case the pain complained of by the subject: instead, it is necessary to evaluate the organism as a whole to get to the real root of the problem.In the first instance, the resolution of the problem will depend on the insults encountered, their correction and the good will of the subject in following the prescribed therapy (whether nutritional, structural or psychological).
Secondly, a "sectorial" reinforcement in the gym of the vastus medialis or the vastus lateralis, as appropriate, is recommended before resuming competitive activity.