to heart cells (transient myocardial ischaemia), which is insufficient to meet the needs of the myocardium.
The reversibility of this condition differentiates angina (or angor, which in Latin means suffocation) from heart attack, a much more serious event which is associated with necrosis (death) of a more or less extensive part of the heart.
Blood is life, since it transports oxygen and nutrients, giving them to the cells and loading itself with waste products. When the blood is scarce, the tissues suffer and accumulate toxic metabolites. This condition is picked up by cardiac chemoreceptors and from there sent to the central nervous system which, by reflex way, triggers the pain sensation. The heart is in fact devoid of sensitive nerve endings.
The blood supply to the myocardium can become insufficient with respect to the needs of the heart itself already in conditions of rest or during physical exertion (climbing stairs, lifting and carrying an object, heavy, etc.). Psycho-physical stress can also favor the unleashing the disease.
The causes of ischemia, in the vast majority of cases, are attributable to coronary diseases. These vessels which, under normal conditions ensure the right blood supply to the heart, can become ineffective in fully satisfying these requests for two main reasons:
- for a reduction of the blood supply to the heart (PRIMARY ANGINA);
- due to an increase in the metabolic demands of the heart (SECONDARY ANGINA).
Primary components
The causes of the onset of "angina pectoris are mainly attributable to:
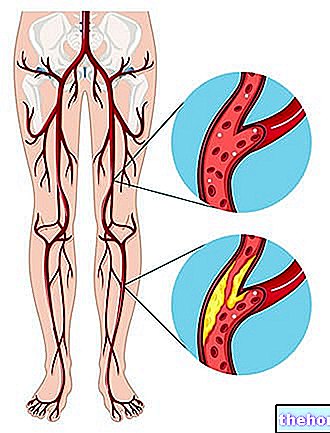
- transient stenosis due to the presence of atherosclerotic plaques. "Atherosclerosis (literally" hardening of the arteries) is a degenerative disease that affects the walls of the arteries by thickening them and decreasing their elasticity. This disease mainly affects large and medium caliber muscular arteries such as coronaries. The consequent hardening of the vessels associated with the formation of atheromas or atherosclerotic plaques is the most common cause of the onset of ischemic heart disease.
- transient coronary spasm that reduces the vessel lumen in healthy arteries (spasm in the absence of stenosis), due to alterations in the normal mechanisms of vasoconstriction and vasodilation.
At the origin of angina there may also be different pathologies such as:
- Severe anemia
- Tachycardia
- Hypertensive crisis
- Heart disorders (hypertrophic myocardiopathy)
- Heart valve disorders (mitral stenosis)
Secondary components
The anginal attack can also arise at rest but generally occurs in situations in which the myocardial demands for oxygen increase:
- physical efforts (more or less intense depending on the severity of the disease)
- stress
- cold shot
- fright
- anger
- intense emotions
- sexual intercourse
- heavy meals
- combinations of these factors
Often angina pectoris is due to the simultaneous presence of both primary and secondary causes aggravated by triggering factors such as intense physical effort. Some patients, as we have seen, already experience pain at rest (in this case we speak of spontaneous angina, class of high risk) while others suffer from angina only in predictable situations such as intense physical activity (exertional angina low risk class).
Between these two extremes lies mixed angina, a form characterized by anginal episodes both at rest and under exertion (medium risk class).
Angina pectoris is a clinical picture characterized by the appearance of chest pain following secondary myocardial ischemia, almost always linked to coronary atherosclerosis.
(or Pre-Infarct Syndrome) .
It is the most common form of the disease and is therefore also referred to as typical angina pectoris. It generally occurs during physical exertion and in general in all those situations that require a greater flow of blood to the heart. In these cases the severity of the symptoms is constant and does not worsen significantly with the passage of months.
In addition to being the most common form, stable or exertional angina is also the least severe, since acute episodes are predictable in frequency and intensity and for this reason can be treated with specific medicines capable of preventing or stopping the attack. .
Unstable angina
It includes different forms of angina pectoris united by the instability of the clinical picture. The two most important characteristics of this form of angina are the recent onset (<1 month) and the "worsening", or the worsening in duration and intensity of the anginal episodes.
With the passage of time, the attacks also occur due to physical exertion of a modest entity (reduction of the ischemic threshold), up to already appearing in conditions of absolute rest. In this case, the therapeutic control is difficult since the patient himself is unprepared to face the anginal attack.
Of the two forms, unstable angina is the most dangerous and is placed in severity between the stable form and myocardial infarction (incidence of AMI in 2% - 15% of cases).
- Constant pain in quality, localization, irradiation and duration, stable over time (appeared for more than a month)
- Exercise angina caused by the discrepancy between the demand and supply of O2 to the myocardium
- Recent angina (less than one to two months)
- Worsening angina (painful fits that get worse over time)
- Angina at rest or with minimal exertion
Unstable angina in turn is divided into two subspecies:
- silent ischemia
- l "angina variant of prinzmetal
Angina or Silent Ischemia
It is a transient condition in which there is a discrepancy between the consumption and the supply of oxygen to the myocardium. Unlike the other forms of angina, silent ischemia is characterized by the absence of symptoms, therefore of pain (hence the name silent = silent) This condition, typical of diabetics, can therefore only be diagnosed by specific tests.
The real causes of the absence of pain have not yet been established with certainty, although they are probably closely related to an increase in the synthesis and secretion of endorphins (endogenous painkillers) by the central nervous system. Even the same heart attack, such as silent angina, is not painful in about 15% of cases.
Variant angina pectoris or Prinzmetal's
It is a rather rare clinical picture, characterized by the appearance of angina at rest and not during demanding physical exertion.
Usually the anginal attack tends to always occur at the same time of day, often at night. Variant angina pectoris is caused by excessive spasm (contraction or narrowing) of the coronary arteries which in many cases are devoid of arteriosclerotic plaques.
transitory or both.SECONDARY ANGINA
It arises secondary to an increase in the myocardial demand for oxygen (classically in relation to exertion), which exceeds the possibilities of replenishment by the coronary flow.
FUNCTIONAL ANGINA
It groups all those situations in which angina is not caused by a coronary artery problem but by other diseases that prevent the heart from receiving the right amount of blood. This group of pathologies includes stenosis and aortic insufficiency, mitral stenosis, severe anemia, hyperthyroidism and severe arrhythmias.
Vasospastic angina, favored by the abuse of cocaine, also falls into this form.
Descriptive criteria
Each individual anginal attack is typically classified according to its:
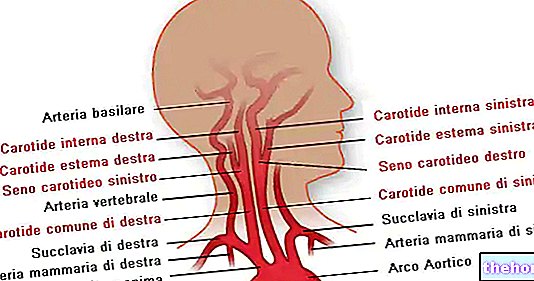
- LOCATION: typically referred to the mid-superior posterior-sternal region; in some cases it can affect the entire thoracic area and radiate to the neck, jaw, left upper limb, fingers and shoulders.
- QUALITY: oppressive, constricting, burning or suffocating varying from mild to severe, generally not modifiable with breaths and position variation.
- DURATION: from a few seconds to 15 minutes; if the anginal pains exceed 20-30 minutes it is probably a myocardial infarction.
- FREQUENCY: sporadic, regular, irregular, frequent.
COLD ANGINA
Caused by exposure to low temperatures and due to coronary vasoconstriction and increased blood pressure.
POSTPRANDIAL ANGINA
It usually occurs after modest effort only when done after a meal and may suggest the presence of severe coronary artery disease.
STRESS ANGINA
Mainly connected to situations of emotional stress.
ANGINA FROM DECUBITUS
Caused by the assumption of the clinostatic position, which increases the cardiac work by increasing the preload.
SYNDROME X or microvascular angina
It is an anginal syndrome characterized by episodes of myocardial ischemia in the absence of atherosclerotic lesions.
Also in this case there is a dysfunction that causes excessive spasm (constriction) of the coronary arteries due to alteration of the normal mechanism of regulation between vasoconstriction and vasodilation. Small arterial resistance coronary vessels are affected.
The risk of angina developing into more serious cardiac events is very low in this case.
The most common symptom of the disease is chest pain which is usually constricting. In these cases, the subject affected by angina feels a strong sense of oppression as if the chest were tightened by a vice. Other times the pain is less intense, vague and more like a nuisance. There is usually a gradual increase in painful intensity followed by progressive fading.
In some cases the pain can extend to the left arm from the ulnar side, to the fingers, and sometimes to the jaw, throat, and stomach. Pain following angina is not affected by breathing or body position.
In general, this symptomatology is aggravated by physical activity, cold air, stress and all other situations in which the heart's energy demands increase considerably compared to the condition of rest. In less severe situations, this pain subsides or simply disappears with rest. Administration of trinitrine relieves pain in most cases.
Other characteristic but not always evident symptoms of angina pectoris are:
- Dyspnea, with a feeling of suffocation
- Sweating
- Nausea
- He retched
These symptoms are not exclusive to angina which can sometimes be confused with other pathologies characterized by similar symptoms. Gastroesophageal reflux can, for example, cause retrosternal pain similar to that of angina; in the same way, neck pain can radiate to the shoulders and arm as it happens in some subjects affected by angina. Biliary colic, esophageal spasms, peptic ulcers (gastric localization) and painful infectious rheumatological syndromes can also cause chest pain.
, saturated fats, simple sugars and cholesterol; diet lacking in fiber, vitamins, fish and polyunsaturated fatty acids in general)GENETICS
- familiarity of the pathology, presence of heart and non-congenital diseases
METABOLIC SYNDROME
- Arterial hypertension (> 140/90 mmHg)
- Obesity (mostly visceral, BMI> 35, waist circumference> 102 in males,> 0.88 in females)
- Diabetes mellitus (insulin resistance)
- Hypercholesterolemia (total cholesterol> 200 mg / dl, good HDL cholesterol <40mg / dl in men or <50mg / dl in women)
In the most serious cases, an intervention is required which can be either percutaneous (angioplasty) or surgical (aortocoronary bypass).
Other articles on "Angina Pectoris"
- Angina - Medicines for the treatment of Angina Pectoris
- Angiography
- Angioplasty