Definition

Mastoiditis occurs when the purulent infection extends from the middle ear (already affected by otitis media) to the mastoid air cells: this infectious process is responsible, precisely, for the inflammation of the mastoid and surrounding tissues.
A degeneration of mastoiditis could lead to the destruction of the bone: from what has been said, it is clear that immediate medical intervention is essential to minimize the risk of complications, often irreversible.
Glossary
Terminology
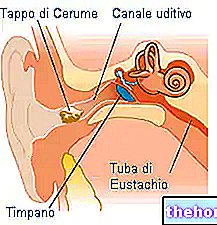
- Mastoid process: lower extension of the petrous rock of the temporal bone of the skull; its function is to act as an anchor for the neck muscles
- Air cells: they are contained in the mastoid process and, within two years of life, develop from the antrum (the only main cavity). The air cells are connected posteriorly to the posterior cranial fossa, and superiorly to the middle cranial fossa.
- Ear tympic cavity: connects the middle ear with the mastoid antrum (thanks to a small canal that crosses the petrous temporal)

Causes
Otitis media, acute or chronic, is one of the etiopathological factors most involved in the onset of mastoiditis. The infection can spread from one ear through the mastoid bone of the skull which, filling with infected material, could deteriorate.
In addition to otitis media, other diseases have been identified that can predispose a patient to mastoiditis.
- intracranial abscess
- meningitis (especially those caused by pneumococcus)
- facial nerve paralysis
- cavernous sinus thrombosis
The pathogens most involved in mastoiditis are: Streptococcus pneumoniae, S. pyogenes, Staphylococcus spp., Haemophilus influenzae, Pseudomonas aeruginosa. On the other hand, Aspergillus and other fungi are pathogens which only rarely favor the inflammation of the mastoid cells.
Mastoiditis can be classified into two variants:
- Acute mastoiditis: pathological process of a suppurative type, essentially due to an acute "otitis media
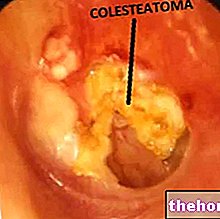
- Chronic or latent mastoiditis: inflammation of the mastoid cells secondary to a chronic inflammatory-suppurative process of the ear or to a cholesteatoma
Terminology
- Suppurative process: pathological process in which there is the formation of purulent material (pus) in an inflamed tissue
- Cholesteatoma: squamous epithelium that originates during chronic "otitis media
Since the air cells are connected posteriorly to the posterior cranial fossa, and superiorly to the middle cranial fossa, any suppuration of the mastoid can cause meningitis or brain abscess.
Risk factors
Some risk factors have been identified that can predispose the patient to the onset of mastoiditis. Infantile age (especially infants 6-13 months), impaired immune system and a previous history of cholesteatoma may make the patient more susceptible to mastoiditis. It has also been observed that patients with speech difficulties or with mental handicaps tend to be more affected by mastoiditis, possibly due to their inability to correctly communicate symptoms and express themselves.
Incidence
Currently, mastoiditis is a rather rare infectious-inflammatory process. However, prior to the introduction of antibiotics, the disease was a fairly common condition, especially in children. In the past, mastoiditis - diagnosed in 5-10% of children with acute otitis media - had an "average incidence of 2 children for every 100,000 healthy. Currently, the mortality rate is estimated to be extremely low (0.01 per 100,000 children).
Clearly in developing countries, where drugs (especially antibiotics) are not very available, the mortality rate from mastoiditis is significantly higher.
Symptoms
For further information: Mastoiditis Symptoms
In general, the symptoms that are often associated with mastoiditis are: mood alteration (irritability), headache, fever lasting more than 4 days, ear pain, gastrointestinal symptoms (vomiting and diarrhea are often the only observable prodromes in affected infants. ).
In addition to these symptoms, mastoiditis is accompanied by a number of characteristic signs, such as retro-auricular edema associated with erythema and fluctuation of the mastoid. The clinical picture of mastoiditis is also marked by all the characteristic symptoms of otitis media.
Acute and chronic mastoiditis
In the table, the typical symptoms of the acute and chronic form of mastoiditis are reported in more detail.
Abnormal protrusion of the outer ear forward (fluctuation)
Swelling and redness of the back of the ear
Swelling and erythema of the tympanic membrane
Lack of appetite
Irritability
Otalgia
Perforation of the eardrum
Crying (in the child)
Previous history of otitis media (acute or recurrent)
Recurrent attacks of ear pain and retro-auricular pain
Recurrent headache
Fever (sporadic episodes)
Infection (obvious or not) of the tympanic membrane
Irritability and crying in infants
Lack of obvious inflammation of the peri-mastoid
Complications
When not treated in time, mastoiditis can create various complications:
- septic arthritis
- brain abscess
- Bezold's abscess (spread of purulent material from the mastoid process - along the digastric muscle - to the neck muscles)
- abscess between the periosteum and the "mastoid bone (cause" of the "protruding eye")
- bone erosion
- zygomatic mastoiditis (extension of the infection in the cheekbone)
- osteomyelitis
- cranial nerve palsy
- hearing loss
- spasm of the carotid artery
- death (rare)
Diagnosis
For the diagnosis of mastoiditis, examination of the head can reveal the characteristic signs; to ascertain mastoid cell infection, it is essential to check for retro-auricular swelling, cervical stiffness and fluctuation of the auricle. The most used diagnostic tests are: blood count with formula (to highlight leukocytosis) and mastoid x-ray. The CT examination is instead reserved for severe cases, in which a spread of the infection to other sites is suspected. The antibiogram, on the other hand, is useful in case of presumed hearing loss.
In patients suspected of mastoiditis, differential diagnosis with infectious cellulitis, bone cysts, fever of unknown origin, lower skull fractures, swelling of the parotids, enlarged cervical lymph nodes, otitis media or externa, intracranial sepsis and trauma is necessary headset.
Treatment
Being a mostly bacterial infection, antibiotics are the therapy of choice for the treatment of mastoiditis; in general, penicillins, cephalosporins and macrolides are the most effective drugs. Eventually, in case of moderate-severe pain and inflammation, the administration of therapeutic aids such as opioids or NSAIDs (eg ibuprofen) is recommended. Paracetamol is also used in therapy to lower fever in the context of mastoiditis.
In addition to antibiotic therapy, some patients must undergo stronger treatment: surgical drainage or mastoidectomy (useful in cases of mastoid osteitis, abscesses, intracranial extension of the infection and cholesteatoma). Surgery is necessary in case of ascertained disappearance of the intracellular mastoid septa, developed during the suppurative process of mastoiditis.