Little sodium in the blood
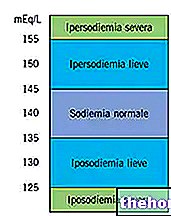
Hyponatremia represents a clinical condition in which the sodium concentration in the blood is lower than normal. Under physiological conditions, the sodium concentration in the blood (natriemia or sodemia) is maintained at levels between 135 and 145 mmol / L. Yes speaks of hyponatremia (or hyponatremia) when this value falls below 135 mmol / L.
In the previous article concerning hyponatremia we focused attention on the possible triggering causes. In this concluding discussion we will analyze the symptoms that distinguish hyponatremia, the diagnostic options and treatments currently available.
Symptoms
In hyponatremia, serum sodium concentrations are reduced, therefore there is an osmotic displacement of water FROM the extracellular to the intracellular compartment. The immediate consequence of this event is cytoplasmic swelling.
Medical statistics show that for sodium levels greater than 125 mmol / L and less than 135 mmol / L (mild hyponatremia) the symptoms are mild, vague, or completely absent. When present, the affected patient complains of gastrointestinal symptoms, especially nausea and vomiting. At lower sodium concentrations, the symptoms are accentuated. In such situations, the following symptoms are often documented:
- Hallucinations
- Ascites (severe form)
- Ataxia
- Convulsions
- Muscle cramps
- Muscle weakness
- Disorientation
- Epilepsy
- Hypotension
- Headache
- Loss of consciousness
- Temporary memory loss
- Slowing of reflexes
- Dry mouth
- Intense thirst
- Severe sleepiness
- Tachycardia
In severe cases, hyponatremia can lead to coma, respiratory depression and death.
More in detail: what happens after a few hours from the onset of hyponatremia?
The organism reacts with an adaptive response: the elimination of electrolytes from brain cells is favored. A similar mechanism is important to limit as much as possible the entry of water into the intracellular site.
In the absence of treatment, after a few days there is a cellular loss of molecules osmotically active (myoinositol, glycerophosphorylcholine, phosphocreatine / creatine, glutamate, glutamine and taurine).
The risk of permanent neurological complications is greater the FASTER is the loss of these molecules:
- Chronic hyponatremia → sodium levels gradually decrease over a few days / weeks → more moderate signs and symptoms
- Acute hyponatrienia → blood sodium levels drop sharply: dangerous potentially fatal effects (brain swelling, coma, death)
Hyponatremia must be considered a serious pathological phenomenon, especially affecting the CNS: cellular edema can exert compression on the brain parenchyma, leading to coma and death.
Diagnosis
Simple medical history and physical examination are not sufficient to ascertain a suspicion of hyponatremia. For diagnostic confirmation, blood and urine tests must be performed.
The assessment of sodemia is certainly one of the most widely used tests: hyponatremia is confirmed when the sodium levels in the blood fall below 135 mmol / L.
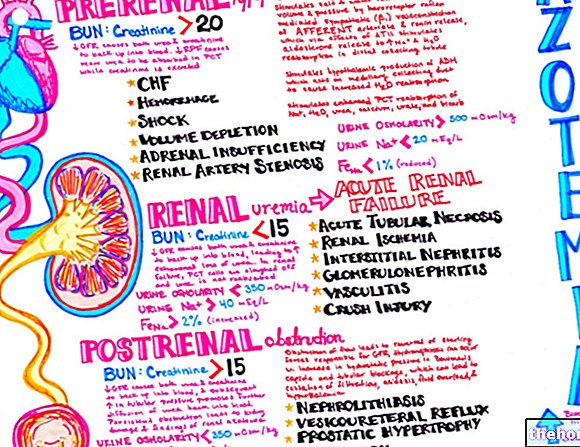
The detection of sodium in the urine> 20 mmol / L indicates hyponatremia due to renal decompensation / pathology and / or the hormones that regulate its activity.
After ascertaining the alteration of sodemia, it is necessary to proceed with a differential diagnosis of hyponatremia to trace the triggering cause.
In some clinical situations, imaging tests may be useful: in the context of congestive heart failure, a chest X-ray is particularly suitable for ascertaining hyponatremia. Brain CT may also be required in patients with obvious impaired consciousness.
Therapies
In addition to being poorly tolerated by the patient, therapies for acute and chronic forms of hyponatremia are often ineffective.
The choice of treatment for hyponatremia is dictated by the underlying cause and the severity of the condition.
Mild or moderate chronic hyponatremia, caused by the abuse of diuretics or by an exaggerated administration of water, should be treated by correcting the dosage of the drugs and limiting the intake of liquids → WATER RESTRICTION
Different speech must be addressed for severe and acute forms of hyponatremia:
- Intravenous administration of a sodium-based solution (hypertonic saline solutions)
- Hormone therapy: indicated for forms of hyponatremia dependent on Addison's disease (insufficiency of the adrenal gland)
- Administration of vasopressin receptor antagonists (reserved for patients with hyponatremia associated with liver cirrhosis, congestive heart failure and SIADH). Tolvaptan (eg Samsca) seems to be particularly effective: start therapy with a drug dose of 15 mg, to be taken once a day. It is possible to increase the dose up to 60 mg / day in order to achieve an adequate level of sodium and volume in the blood.
- Administration of demeclocycline or lithium: indicated in the context of hyponatremia associated with SIADH. These drugs reduce the responsiveness of the collecting tubule to ADH.