Definition of erysipelas
"Erysipelas" is a term extracted from medical language that identifies an "acute infection of the skin, with evident involvement of the dermis, the superficial layers of the hypodermis and lymphatic vessels:" erysipelas is generated by a "bacterial infiltration responsible for progressive maceration of the skin, in turn favored by micro-lesions in the skin.
Incidence

Causes
Many studies have been carried out to find out what the main cause was: it seems that the causes of erysipelas are the beta-haemolytic streptococci of type A, but other bacterial strains implicated in the disease have also been isolated. In fact, it seems that Streptococcus piogene, staphylococci, staphylococci of groups B, C and G, and other gram-negative bacteria contribute to the formation of infectious bubbles, sometimes of a haemorrhagic nature. Evidence-based dermatology, by Luigi Naldi, Alfredo Rebora].
Symptoms
For further information: Erysipelas Symptoms
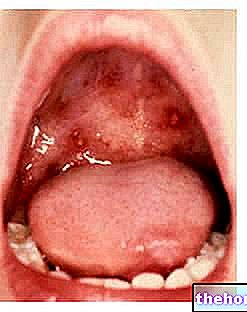
Erysipelas tends to spread to some peculiar areas: face, legs and arms are the most common loci of infection. Some texts define the onset of the disease as "dramatic", characterized by alteration of body temperature (low-grade fever or high fever), sensation of cold and chills, headache and perception of local burning, followed by the real clinical manifestations of the disease.
Patients with erysipelas have shiny red spots (erythematous patches) on the skin, slightly raised, slightly warm to the touch; the affected areas appear swollen, sometimes painful under pressure. Often times, erysipelas degenerates forming pustules, bubbles, blisters and itching. The culprits are mostly streptococci which, once penetrated through the small wounds of the skin, reach the lymphatic vessels where they cause exudation and inflammation, also affecting the glands surrounding lymphatics (eg the inguinal lymphatic glands are potential targets of erysipelas, especially when the infection affects the lower limbs). Some subjects with erysipelas present skin necrosis of the areas affected by the infection, as well as succulent and itchy blisters.
Generally, on the face, erysipelas infects the nose, cheeks and eyelids, causing eyelid edema, itchy and succulent blisters, and possible conjunctival discharge. [From Infectious diseases by Mauro Moroni, Roberto Esposito, Fausto De Lalla].
Risk factors
It is believed that the onset of erysipelas and its subsequent degeneration are favored by some risk factors: obesity, diabetes mellitus, deep venous insufficiency, lymphedema in the legs, tinea pedis, microlesions, wounds, insect bites, responsible - the latter - of the laceration of the skin, a possible access route for bacterial colonization.
Complications of erysipelas
Fortunately, complications are rare, albeit possible: it is estimated that only in 1% of patients with erysipelas, the disease degenerates into endocarditis at the level of the aortic valve.
In other cases, erysipelas could evolve into abscesses, glomerulo-nephritis (renal inflammation) or secondary pneumonia (extremely rare event). We mentioned that erysipelas could involve the lymphatic vessels, so any worsening of the disease could cause severe patients, elephantiasis.
Furthermore, the umbilical scars of the newborn could act as gateways for the proliferation of staphylococci: consequently, the infected scar could cause a serious infection to the newborn, which appears cyanotic, suffering and jaundiced.
When the bacteria enter the bloodstream, they could generate severe sepsis (septicemia), due to the streptococcal colonization in the blood and the proliferation of toxins of the same.
Surely, the most serious complication of erysipelas is necrotizing fasciitis (rare bacterial inflammation of the deep skin and subcutaneous layers).
Other complications of erysipelas include: osteitis, arthritis, tendinitis, thrombosis of the venous sinuses. [Taken from Evidence-based dermatology by Luigi Naldi, Alfredo Rebora].
Diagnosis
Generally, to diagnose erysipelas, the doctor uses a simple physical examination (clinical diagnosis); for a "further diagnostic confirmation, some indicators of bacterial inflammation (eg procalcitonin) are useful, although the isolation of the pathogenic bacteria," sometimes, it's not that simple.
In some cases, the diagnosis could be wrong: in order to overcome this problem, the biopsy could be a valid diagnostic test, useful for distinguishing erysipelas from other non-infectious diseases, but of an inflammatory nature (eg erysipelas carcinoma). When the diagnosis is wrong, an inflammatory breast cancer could be mistaken for "simple" erysipelas.
The clinical manifestations caused by erysipelas should not be confused with those caused by herpes zoster or contact dermatitis.
Care
For further information: Medicines for the treatment of Erysipelas
Shock therapy useful for fighting bacterial infection is based on the administration of antibiotics: when the responsible bacterial strain is isolated, the patient is prescribed specific antibiotics, including benzylpenicillin benzatin (or clindamycin, if the patient is allergic to penicillin), macrolides (e.g. erythromycin) and cephalosporins in general.
The use of NSAIDs (Non Steroidal Anti-Inflammatory Drugs) is absolutely forbidden in case of erysipelas, as it could potentially favor the progression of the infection into more complicated forms.
Generally, the improvements are almost immediate: the responsible bacterium is eradicated, so the patient heals from erysipelas within a few days.
Relapses of erysipelas are possible: in such situations it is advisable to keep the patient under control, who are generally prescribed specific pharmaceutical specialties for the prophylaxis of relapses (eg mycotic erysipelas).
Summary
To fix the concepts ...
Illness
Erysipelas
Description of the disease
Acute cutaneous infection, with evident involvement of the dermis, hypodermis and lymphatic vessels
Incidence
Typical childhood and senescence disease
Little widespread in Italy
Common in France (10-100 cases per 100,000 healthy subjects)
Etiological research
- Beta-haemolytic type A streptococci (the main culprits)
- Streptococcus pyogenic, staphylococci, staphylococci of groups B, C and G and other gram-negative bacteria
Anatomical areas most affected
- Face (nose, cheeks and eyelids)
- Legs
- Arm
Clinical manifestations
Onset: dramatic with fever, cold, chills, local burning
Evolution: swollen and erythematous patches on the skin, pustules, blisters, blisters and itching
At the level of the lymphatic vessels: exudation and inflammation
Degeneration of the disease: skin necrosis of the areas affected by the infection, as well as succulent and itchy blisters, eyelid edema, possible conjunctival secretion
Risk factors
Obesity, diabetes mellitus, deep vein insufficiency, lymphedema in the legs, tinea pedis, microlesions, wounds, insect bites
Complications
Rare but possible: aortic valve endocarditis, abscesses, glomerulo-nephritis (renal inflammation), secondary pneumonia, elephantiasis, severe infection in the newborn, septicemia due to streptococcal colonization in the blood, necrotizing fasciitis, osteitis, arthritis, tendinitis, thrombosis of the venous sinuses
Diagnosis
- clinical diagnosis
- biopsy
- bacterial inflammation indicators (eg pro-calcitonin)
Therapy against erysipelas
Once the responsible bacterial strain is isolated, the patient is prescribed specific antibiotics:
- cephalosporins
- benzylpenicillin benzatin
- macrolides