Generality
Alopecia, or localized or diffuse hair loss, is a phenomenon that affects large sections of the population, both men and women.
In the most common and widespread form, hair loss is linked to the action of androgens on a genetically predisposed ground; we therefore speak of androgenetic alopecia.

In women, hair loss, although generally more attenuated than in men, often involves much more dramatic and devastating psychological repercussions, linked to the perception of considerable damage to one's image. Fortunately, the treatment of female androgenetic alopecia offers greater and more effective therapeutic opportunities, with a lower incidence of side effects.
Causes
An essential element in all forms of androgenetic alopecia is - as the name itself suggests - the presence of androgens. In fact, in the absence of these hormones - as is appreciated in precociously neutered males - baldness does not manifest itself.
In the article dedicated to the relationship between androgens and hair, however, we explained how hormone levels are quite similar in bald men compared to the general population. Male androgenetic alopecia, therefore, is generally not related to excess androgens, but rather to "excessive sensitivity of the hair follicles to their action. In fact, from birth, some hairs are genetically predisposed to receive the "miniaturizing" stimulus of androgens. Not surprisingly, androgenetic alopecia is a slow phenomenon which - by shortening the growth phases more and more and lengthening those of rest before the fall - involves the gradual transformation of the terminal hair into pixie hair (thin, depigmented, very short and almost imperceptible ).
As explained above, women suffering from hyperandrogenism (excess of androgens) are clearly more susceptible to alopecia, even if the two conditions are not always and necessarily correlated. Women suffering from acne, seborrhea, hypertrichosis and hirsutism (suggestive signs but not pathognomic of hyperandrogenism), are therefore more likely to suffer from female alopecia.
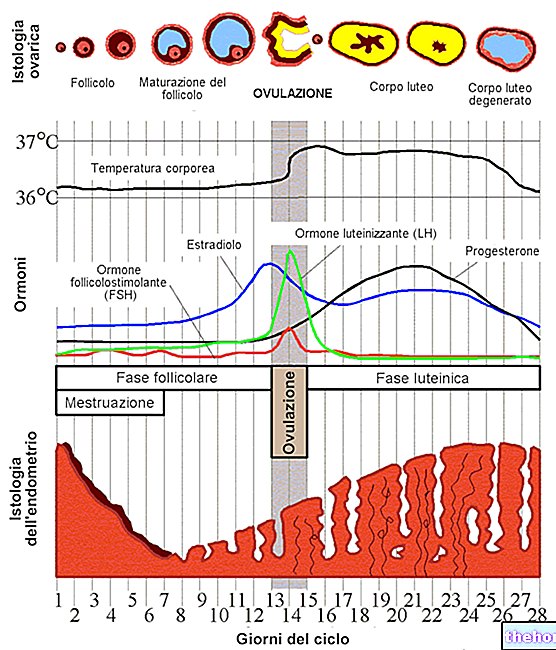
In women, most cases of hyperandrogenism are attributable to polycystic ovary syndrome (PCOS), which clinically manifests itself with anovulatory cycles, menstrual changes, hirsutism and sometimes obesity. consequently, either as a trigger, to states of hyperandrogenism, probably favored by the variable degree of insulin resistance related to it. On the other hand, cases of hyperandrogenism linked to the presence of androgen-secreting neoplasms are rarer.
Even the levels of estrogen, hormones that unlike androgens are typical of women, especially during the fertile age, influence - this time positively - the health of the hair.
Furthermore, at the level of the hair bulbs and capillaries, there may be variable concentrations of enzymes acting on androgens and estrogens, which transform them into derivatives capable of influencing the life of the hair to a much greater extent. The best known of these enzymes is called 5-alpha-reductase and acts on testosterone transforming it into dihydrotestosterone, the real responsible for the involution of the hair and the consequent thinning.
The aromatase enzyme, on the other hand, converts androgens into estrogens, prolonging the life of the hair and counteracting baldness; a similar action is also performed by the 3-alpha-steroid dehydrogenase and 17-beta-hydroxysteroid dehydrogenase enzymes. For this reason, female androgenetic alopecia can be noticed for the first time, or become more evident, after menopause, a time when there is a generalized decrease in estrogen with a variation in the percentage ratio between ovarian and adrenal steroids. always necessary genetic predisposition, the same circumstance can therefore manifest itself in coincidence with hormonal changes, due, for example, to a birth or to the beginning or interruption of estrogen-progestin treatments (including those for contraceptive purposes.
Symptoms and Features
The hereditary component is "another distinctive feature of" androgenetic alopecia; consequently, the problem is much more likely to be accused when it has already made itself evident in parents, grandparents, uncles or siblings.


Diagnosis
In women, the precocity of diagnosis and therapeutic intervention is very important to stop the process of involution of the follicles, making the hair regain its original splendor before the problem becomes irreversible.
The pivotal examination for the diagnosis of female alopecia is the trichogram, naturally flanked by the inevitable anamnesis and the evaluation of the clinical picture.
In particular, the familiarity of alopecia, the intake of contraceptive or cortisone pills, the possible use of anabolic steroids and the regularity of the menstrual cycle will be evaluated, looking for possible signs of hyperandrogenism (lowering of the voice, hair diffused in typically male areas, obesity, acne etc.).
To confirm or exclude what emerges from the anamnestic data and from the physical examination, it is necessary to proceed with endocrinological laboratory screening, during which the blood concentrations of androgens, cortisol, thyroid hormones, TSH, SHBG, estrogen, progesterone and gonadotropins (LH , FSH), also in relation to the various phases of the menstrual cycle.
Only in this way will it be possible to intervene pharmacologically on the delicate hormonal balance of the woman, improving the therapeutic efficacy of the treatment and minimizing the side effects.
Treatment
The pharmacological therapeutic options for female androgenetic alopecia, largely impracticable in men, must first of all be divided into topical and systemic ones.
The first group includes drugs to be applied directly on the scalp, such as the famous minoxidil or estrone sulfate. The topical administration of hydroalcoholic solutions of natural progesterone or its 17-hydroxylated derivatives, associated or not with spironolactone, also seems effective in this sense. There is also the possibility of counteracting the activity of the 5-alpha-reductase enzyme by topical application of azelaic acid.
Systemic drug therapy of female androgenetic alopecia is indicated in cases of hyperandrogenism on a dysfunctional basis, as precisely in the case of PCOS; while in hyperandrogenisms sustained by organic causes (for example, from androgen-secreting neoplasms) it is necessary to remove the cause itself by surgical intervention.
Among these drugs we remember the spironolactone which - to limit the side effects associated with the therapy (amenorrhea, mastodynia, chloasma) - must be taken systemically from the 16th to the 25th day of the cycle, better if combined with an estrogen-progestin to guarantee contraception. .
In case of progestogen deficiency, however, the administration of synthetic progestogens by systemic route is indicated.
However, the most commonly adopted therapeutic solution remains the combined administration of estrogens and progestogens, in particular of ethinylestradiol and cyproterone acetate (with important antiandrogenic activities). This therapeutic intervention is exploited not only in the treatment of female androgenetic alopecia, but also in the treatment of the manifestations of hyperandrogenism in women.
For further information: Drugs for the Treatment of "Female Androgenetic Alopecia"
Other articles on "Female Alopecia"
- Androgenetic alopecia
- Alopecia
- Norwood and Ludwig scale and androgenetic alopecia
- Alopecia areata
- Alopecia - Medicines for the treatment of Alopecia
- Alopecia: natural remedies for hair loss













.jpg)