In the previous video we talked about thyroid nodules and the fact that in a small percentage of cases they can assume malignant tumor characteristics. Today we will investigate precisely this aspect and we will see in more detail what thyroid cancer is and what forms it can take.
Like other organs, the thyroid gland can also be affected by benign and malignant tumors. In the latter case, we speak more properly of cancer. Fortunately, in the vast majority of cases, these tumors are poorly aggressive and treatable with relative ease; in fact, they have a less severe clinical course than many other neoplasms affecting other organs.
Benign thyroid tumors are in the majority of cases adenomas. These result from the abnormal growth of a group of cells, localized and separated from the remaining healthy thyroid tissue by a fibro-connective capsule.
In some cases, benign thyroid nodules can cause hyperthyroidism. When this happens we speak of a toxic adenoma or "Plummer's disease". Benign thyroid tumors are associated with a positive prognosis and, unlike malignant ones, do not spread throughout the body and therefore do not metastasize.
Only a small percentage of thyroid nodules, about 5%, hide malignant tumors. These can be divided into four main forms, different both for the type of cells from which they are composed, and for aggressiveness and prognosis. These four cancers are papillary carcinoma, follicular carcinoma, medullary carcinoma and, last but not least, the most aggressive, anaplastic carcinoma.
There are also cases, quite rare, in which those of the thyroid gland are tumors of metastatic origin and therefore originate from other organs, lymphomas, i.e. tumors of lymphatic origin, or sarcomas, deriving from the muscular or cartilaginous tissues surrounding the gland.
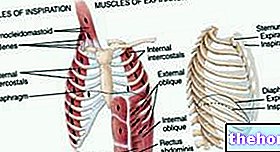
Papillary and follicular carcinoma originate from the follicular cells that make up the gland tissue. These cancers, also called differentiated, make up about 90% of malignant thyroid tumors. The difference between the two is that the tumor cells of follicular carcinomas blend better with normal ones, making diagnosis more difficult, and are more aggressive than those of papillary carcinomas. Precisely in this regard, it should be noted immediately that differentiated carcinomas of the thyroid, if treated adequately, have a very good prognosis.
Much rarer than the differentiates are medullary and anaplastic carcinoma. Medullary carcinoma arises from calcitonin-secreting parafollicular cells and is often associated with other endocrine problems.
The most aggressive and dangerous form, but fortunately rarer, is the so-called anaplastic or undifferentiated carcinoma. This malignant tumor causes a rapid and painful enlargement of the thyroid gland, tends to invade nearby structures, causes early metastases and is very difficult to treat.
Thyroid cancer is the most frequent endocrine cancer and various risk factors seem to favor its onset. Among these, we recall the exposure to ionizing radiation, accidental or for therapeutic purposes. Among the ascertained risk factors there is also goiter, that is the benign growth of the gland, which, in some cases, can predispose to the transformation of cells in a neoplastic sense. Furthermore, again with regard to thyroid pathologies, there is an important association between Hashimoto's thyroiditis and malignant thyroid lymphoma.
Family history of thyroid cancer is also an important risk factor to consider. In particular, medullary carcinoma may be associated with a syndrome, called multiple endocrine neoplasia type 2 (or MEN 2), which has a genetic basis.
Finally, thyroid cancer is more common in women than men and the risk increases with advancing age.
The conditions that can lead to suspicion of thyroid cancer are different. One of the most common is the identification of one or more nodules by palpation of the anterior region of the neck, corresponding to the gland. However, it must be remembered that not all thyroid nodules hide forms of cancer. Indeed, they are often simply a sign of the so-called thyroid hyperplasia, which is benign excessive growth of the thyroid tissue.
A thyroid tumor is more likely to be malignant if the lump reaches the size of a mass. Sometimes, the first sign to appear is an enlarged lymph node. In other cases, there is a feeling of oppression in the neck.
Late-stage symptoms may include changes in the voice and difficulty swallowing and breathing, due to the involvement of adjacent neck structures. A neoplastic nodule can also be associated with the symptoms of hyperthyroidism or hypothyroidism.
After finding a thyroid nodule during a physical exam, the doctor generally prescribes a series of tests to measure thyroid function and identify any pathological alteration in hormone levels. Blood tests, therefore, include the measurement of thyroid hormones and TSH, although often, in the presence of a thyroid tumor, these levels are normal. The determination of calcitoninemia, on the other hand, serves to exclude medullary carcinoma, which is characterized by the presence of high circulating levels of calcitonin.
Moving on to instrumental investigations, today the simplest and most specific exam to study the thyroid is ultrasound. This allows to identify the relationship of the nodule with the gland and with the surrounding tissues; moreover, it allows to recognize some characters of benignity or suspected malignancy. Another very useful test is the thyroid scintigraphy, which allows to define the nodule based on its endocrine activity. This is possible thanks to the administration of an iodinated radioactive contrast medium which is accumulated by the thyroid tissue with a strong or weak affinity. In other words, the thyroid nodules, compared to normal tissue, can be hypercaptive or hot, if they accumulate more radioactive isotope than the surrounding tissue; in this case they appear very colored on scintigraphy; on the contrary, nodules that do not incorporate radioactive iodine are defined as cold. Hot thyroid nodules, as a rule, are not malignant, while cold nodules can hide a tumor. One of the methods used to confirm the diagnosis of thyroid cancer with certainty is cytological examination using fine needle aspiration. During this procedure, a fine needle is inserted through the skin under ultrasound guidance to take a sample of material from the lump, which is then examined under a microscope. A further diagnostic investigation can be obtained with a CT scan or an MRI, to identify the possible sites of spread of the disease.
The treatment of first choice for the treatment of thyroid cancer is surgery: the removal usually involves the entire gland, as well as any affected lymph nodes. After the operation, as there is no more thyroid, hormone therapy is prescribed. replacement, i.e. based on synthetic thyroid hormones such as sodium levothyroxine. Upon completion of the therapeutic procedures, the patient can undergo radioactive iodine therapy. This treatment, called radiometabolic, allows to eliminate any residual thyroid tissue and prevent metastases. Radioactive iodine, in fact, reaches the cancerous thyroid cells greedy for iodine, which use it to produce thyroid hormone. The radiation emitted by the radioactive isotope, transported to the nucleus of the thyroid cell, destroys it.
As far as chemotherapy is concerned, this is generally limited to tumors that have already metastasized at a distance.