Generality
Laminectomy is the surgery with which the vertebral lamina is removed, in order to reduce the disturbances generated by excessive compression of the spinal cord and / or spinal nerves.

Laminectomy consists in "removing a vertebral lamina thus obtaining an" opening of the spinal canal.
From the site: aimisspine.com
Surgeons use laminectomy only when conservative treatments for spinal stenosis, herniated discs or abnormal curvature of the spine have yielded poor results.
As with any operation performed under general anesthesia, even in the case of laminectomy the patient must undergo a series of clinical examinations and tests and, on the day of the operation, present himself completely fast.
The procedure is delicate and can take several hours; recovery times, as well as results, vary according to the causes of spinal cord compression.
What is a laminectomy?
Laminectomy is a "surgical operation aimed at decompressing the spinal cord and / or spinal nerves, obtained by removing one or more vertebral laminae. For this reason, it is also called decompressive laminectomy or decompression of the spinal cord.
WHAT IS THE VERTEBRAL LAMINA? BRIEF REVIEW OF THE ANATOMY OF THE SPINE
The vertebral column, or rachis, represents the backbone of the human body and is made up of 33 irregular bones superimposed on each other, called vertebrae.

Image from the site: ceufast.com
The spine is made up of:
- 7 cervical vertebrae
- 12 thoracic vertebrae
- 5 lumbar vertebrae
- 5 sacral vertebrae
- 4 coccygeal vertebrae


Images from the site: lancsteachinghospitals.nhs.uk
In general, the vertebrae have a fairly similar basic structure: they are, in fact, all composed of a body (anteriorly) and an arch (posteriorly), similar to a horseshoe.
The vertebral arch, which delimits the hole through which the spinal cord passes (vertebral hole), includes various parts:
- Two peduncles, which in fact form the bases of the arch. The peduncles on the same side of two adjacent vertebrae delimit a space, called the intervertebral hole, in which a spinal nerve passes.
- Two transverse processes
- Two upper articular processes and two lower articular processes
- A thorny process
- Two foils
The laminae (often also indicated by the term in the singular, therefore lamina) are the vertebral bony regions that go from the peduncles to the spinous process and which host the yellow ligaments of the vertebral column. The yellow ligaments, in addition to putting the adjacent vertebrae in communication with each other, also serve to ensure elasticity and flexion capacity to the entire spine.
Between one vertebra and the other, there is a disc of fibrocartilage tissue, called the intervertebral disc, whose function is to absorb shocks and loads that damage the spine. In other words, the intervertebral discs act as small pads.
The entire space that the spinal cord passes through is called the spinal canal.
When you do
The specialist surgeon resorts to laminectomy in the presence of a spinal stenosis. By spinal stenosis, we mean any narrowing of the spinal canal that causes compression of the spinal cord or the nerves that branch off from it.
SYMPTOMS AND CAUSES OF SPINAL STENOSIS
A spinal stenosis causes different neurological deficits, depending on the region of the spinal cord involved and the extent of the compression. For example, if the affected area is the cervical one (cervical stenosis), the disorders will be borne by the anatomical areas controlled by the nerves and from the spinal cord to the cervical area.
The classic symptoms of a spinal stenosis are:
- Ache
- Sense of numbness in the anatomical areas innervated by the affected section of the medulla.
- Muscle weakness
- Loss of control of the anal and bladder sphincters
- Paresthesia
- Lack of control of some voluntary muscles
Possible causes of spinal stenosis:
- Osteoarthritis
- Rheumatoid arthritis
- Chiari malformation and other congenital alterations of the central nervous system
- Syringomyelia
- Trauma to the spine. Following a trauma, a vertebra can shatter and a part of it end up inside the spinal canal.
- Effects of aging (osteoporosis; bone growths inside the spinal canal, cysts close to the spinal nerves, etc.)
- Spinal cord tumors
- Tumors near the spinal cord or spinal nerves
LAMINECTOMY AS THE LAST REMEDY
Typically, laminectomy is done only after conservative treatments for spinal stenosis (drug therapy and physiotherapy) have failed.
This is because laminectomy is a delicate procedure, the complications of which can be very serious.
OTHER USES
Doctors can also resort to laminectomy in case of severe herniated disc or abnormal curvature of the spine. As in the case of spinal stenosis, every other known type of conservative therapy must be tried before surgery.
Risks
Laminectomy is a fairly safe procedure, but, like any surgical operation, it can involve the following complications:
- Hemorrhages
- Infections
- Formation of blood clots in the veins (deep vein thrombosis)
- Stroke or heart attack during the operation
- Allergic reaction to anesthetic drugs or sedatives used during the surgery
Furthermore, since it affects very delicate structures such as the spine and spinal cord, there is a risk (albeit minimal) of:
- Permanent damage to the spinal nerves or spinal cord
- Relapses, or reappearance, after a period of temporary healing, of pain, numbness, etc.
- Reduced improvement in symptoms
- Infections at the level of the operated vertebrae
Preparation
Laminectomy is performed under general anesthesia and therefore requires special preparation.
First of all, the patient undergoes a series of clinical tests (physical examination, blood test, electrocardiogram, etc.) and an evaluation of his clinical history.
After that, the operating surgeon (or a qualified member of his staff) will illustrate the procedures, the possible risks, the pre- and post-operative recommendations and, finally, the recovery times.
Main pre- and post-operative recommendations:
- Before the laminectomy, stop any treatment based on antiplatelet agents (aspirin), anticoagulants (warfarin) and anti-inflammatory drugs (NSAIDs), because these drugs, by reducing the clotting capacity of the blood, predispose to severe bleeding.
- On the day of the procedure, go on a complete fast for at least the previous evening.
- After the surgery, be assisted by a trusted person.
- If you are a smoker, stop smoking at least until the wound has healed completely.
WHY IS CLINICAL HISTORY IMPORTANT?
Evaluating a patient's medical history means questioning him to find out, for example, if he knows he is allergic to some anesthetic drug, if he suffers or has suffered in the past from cardiovascular problems, if he is taking certain drugs and if, in the case of a woman, he is pregnant.
This information is valuable, because it allows you to better plan the procedure.
Attention: those who suffer from diabetes or other pathologies that require a "constant drug intake are required to inform the surgeon of their condition, so that the latter can make the most appropriate changes to the standard procedure.
Procedure
Once in the operating room and lying on the surgical table on his stomach, the patient is connected by the medical staff to a series of instruments for monitoring heartbeat, blood pressure and oxygen levels in the blood.
Once this is done, he is anesthetized and rendered completely unconscious and numb to pain. To take care of the anesthesia is an anesthetist.
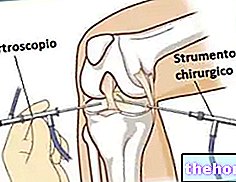
At this point the surgeon intervenes, who begins the actual operation:
- First, it cuts the skin region of the back where the vertebrae (or vertebrae) to be operated on resides, and moves the muscles and ligaments that cover the latter.
- Then, using a highly precise surgical microscope, he dissects the vertebral lamina with extreme delicacy and removes the desired part (N.B: very often the removal also includes the spinous process).
- Finally, he repositions the muscles and ligaments as they were in the beginning and closes the incision with sutures.
Attention: if the laminectomy is aimed at treating a herniated disc or an abnormal curvature of the spine, the surgeon also performs, respectively, a discectomy (ie the elimination of the herniated portion of the disc) or a spinal fusion operation.
DURATION OF THE PROCEDURE
A laminectomy surgery can last from 1 to 3 hours (including anesthesia).
Post-operative phase
Immediately after the laminectomy, the patient is taken to an admission room in the hospital center, where the operation was held, and there he is kept under close observation for several hours.
Based on the assessments of the operating surgeon, discharge can take place on the day of the operation or one or two days later.
After discharge, the patient should start physiotherapy as soon as possible, in order to recover faster and in the best possible way.
WHAT TO DO IN CASE OF PAIN?
After a laminectomy, it is normal to feel pain, so do not be alarmed (unless it is very intense).
To relieve this sensation, doctors recommend taking pain relieving medicines, such as acetaminophen.
RECOVERY TIMES
The complete recovery of the flexibility and mobility of the spine takes place after several months of careful and scrupulous physiotherapy.
During this time, it is possible to resume some of the normal daily activities, as long as they do not involve an excessive load on the spine. The return to work depends on the type of work performed.
In the case of laminectomy combined with spinal fusion, full recovery occurs only after 6-12 months.
Results
In most cases, laminectomy improves the patient's symptoms and quality of life.
However, if the triggering causes are degenerative diseases (such as, for example, in the case of spinal stenosis from osteoarthritis), the original symptoms that forced the operation may recur.
Therefore, the results of laminectomy depend to a large extent on the reasons that made it necessary.











.jpg)











