The cardia is the anatomical region of junction between the esophagus and the stomach, normally located in the abdomen 2 to 4 cm below the diaphragm. Anatomically, the cardia is now considered part of the stomach.

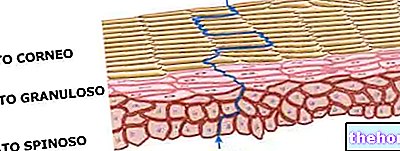
In the cardia we witness the transition between the esophageal and gastric mucosa; at the point of passage, a frayed line (line Z) separates the gastric mucosa, which is redder and more wrinkled, from the esophageal mucosa (at the level of the cardia occurs the passage between two specialized epithelia: the monostratified cylindrical epithelium of the gastric mucosa from one side and the multi-layered pavement epithelium of the esophageal one on the other).
The cardia is innervated by the vagus nerve, which has an inhibiting function, and by afferents of the sympathetic nervous system, which instead have an exciting function. Its biological function is facilitated by the angle of His, the subdiaphragmatic tract of the esophagus, the diaphragmatic crura and the brake-esophageal ligament.

Carcinoma of the cardia is today a growing neoplasm in Western countries; there are numerous possible risk factors, such as alcohol, tobacco and obesity, but the only significantly correlated factor seems to be Barrett's esophagus, a pre-neoplastic condition secondary to chronic gastroesophageal reflux (malignant cardia cancer is therefore more frequent in men compared to women, and in the age groups over 50 years).










.jpg)











