Definition
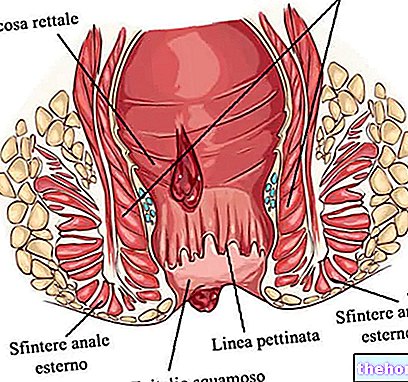
Anal fistulas are small pathological and infected tunnels that connect the anus with the surrounding skin. Specifically, to be defined as such, anal fistulas must develop in the precise anatomical site - called "combed line or anorectal line" - which separates the rectum from the anus, where the exocrine anal glands are housed.
To understand: what are the anal glands?
The anal glands - precisely called glands of Hermann and Desfosses in memory of their discoverers - are tiny anatomical structures located along the wall of the anal canal. Their tubular glandular ducts secrete their contents into the anal crypts (small hollows in the shape of a swallow's nest that are arranged in the anal region in a curiously circular fashion).
Anal fistulas are the final result of an infection of these glands which, as it progresses, degenerates into an abscess.
- In other words, anal fistulas represent the immediate complication of an inadequately treated anal abscess.
How they are formed
We have seen that anal fistulas represent the direct consequence of an untreated "abscess infection (abscess).
To develop the fistula, the infection must originate in the crypt: the pathogens are able to penetrate the sphincter apparatus reaching the crypts of the anal glands.
When the anal glands become inflamed (for example due to the passage of pathogens from the faeces) a pus sac is formed which, when ruptured, gives rise to the anal fistula.
But the process that leads to the formation of the fistula can also be different: in certain circumstances, fecal residues or mucous secretions are blocked in the anal crypts, such as to favor the infection of the glands. In turn, the infectious process can be induced either by "entry of fecal material into the excretory tubules, both from a blockage of the outflow of the glands.
Remember that ...
Anal abscess and anal fistula represent two evolutionary stages of the same disease: the abscess is in fact the acute complication of an infection, while the anal fistula constitutes its chronic form.
- There is no anal fistula without an abscess
Causes and risk factors
Fistulas can be favored by various factors, the same ones responsible for anal abscesses:
- Anal ulcers
- Inflammatory bowel diseases, such as Crohn's disease, diverticulitis and ulcerative colitis. It is estimated that 50% of patients with Crohn's disease experience an anal fistula at least once.
- Impaired Immune System: 30% of HIV patients develop anal fistulas
- Rectal cancer
- Tuberculosis
- Sexually transmitted diseases (e.g. chlamydia and syphilis)
- Complication of bowel surgery
Compared to women, men seem to be more sensitive to anal fistulas. Furthermore, medical statistics show that this disorder occurs with greater incidence in young-adult men aged between 20 and 40 years.
Types of anal fistulas
Anal fistulas are not all the same: they are essentially classified on the basis of structure and location.
Depending on the structure, the following are included:
- Rectilinear fistulas: they have a single communication channel
- Branch fistulas: Multiple connecting channels are observed
- Horseshoe fistulas: connect the anal sphincter to the surrounding skin, first passing through the rectum
On the basis of the location of the fistulous canaliculus, "high" fistulas are distinguished, located above the dentate line, and "low" fistulas, located below. More specifically, anal fistulas can be classified in various ways, but generally reference is made to the Parks classification or to that proposed by the American Gastroenterological Association (AGA).
* A little anatomy to understand ...
The external anal sphincter is a striated muscle consisting of two bundles:
- Subcutaneous bundle *, crossed by fibers of the complex longitudinal tunic
- Deep bundle *, the thickest part of the sphincter that surrounds the mucous membrane of the anal canal and the internal sphincter
The levator anus * is instead a thin and elongated muscle, divided into three sections: pubococcygeal, puborectal and ileococcygeal

- Superficial fistulas: located distally (below) to both the internal anal sphincter and the external sphincter complex (as shown in the figure, they do not cross the internal or external sphincter)
- Intersphincteric fistulas: located between the internal anal sphincter and the external sphincter complex; may extend downward to the perianal skin, upward (blind), or open into the rectum
- Transphinteric fistulas: they pass through the interstitial space and the external anal sphincter; they then pass through both the internal and external sphincter
- Suprasphincteric fistulas: pass through the internal sphincter, pass upward around the external sphincter over the puborectal muscle, then head downward into the levator muscle before making their way to the skin
- Extraspheric fistulas: they have a path that starts above the internal anal sphincter and ends in the external cutaneous orifice.
Signs and symptoms
For further information: Anal Fistula Symptoms
The clinical picture of a patient suffering from anal fistulas includes a tangle of rather obvious signs and symptoms.
If, in the early stages of the disease, the patient does not realize the infection, in the acute phase the symptoms certainly do not go unnoticed. The anal fistulas in fact cause an unpleasant sensation of irritation, itching and swelling in the anal, which tends to become accentuated. during defecation and is typically accompanied by minimal but continuous discharge of stool, pus or mucus, which keeps the anal region moist causing dermatitis and itching. The perceived pain can become unbearable by performing certain movements, so much so that some patients even struggle to stay sitting on a hard surface.
It is not uncommon to see bleeding or pus in the stool; very often, the loss of serous material or pus from the anal orifice also occurs independently of the evacuation (fecal incontinence). In some patients affected by anal fistula there is also a more or less significant rise in body temperature (fever / low-grade fever).
In the absence of a pharmacological or surgical intervention, the typical symptoms of anal fistula can degenerate: the chronic inflammation given by the anal abscess can, over time, predispose to the development of malignant neoplasms.
In severely immunocompromised patients such as those affected by AIDS, the anal fistula tends to degenerate into Fournier's necrotizing fasciitis, thus extending towards the genitals and groin.
Diagnosis
The proctological examination is essential to ascertain a suspicion of anal fistula. After analyzing the symptoms reported by the patient, the doctor proceeds with the physical examination, which can also be performed under local anesthesia.
Although the ascertainment of an anal fistula is rather simple, unfortunately the precise identification of the fistulous path is rather complex; so much "is that very often the entire fistulous path can only be identified during surgery.
Typically, the diagnosis consists of a gentle endoanal ultrasound (performed with a special rotating probe capable of identifying the canal path as much as possible). Here, the doctor will evaluate:
- Local redness and swelling
- Possible blood loss
- Leakage of pus during rectal examination
- Any surgical scars
When anal fistulas are very complex and branched, perianal MRI is often required.
Treatment
Medical treatment of perineal fistulas includes antibiotics, immunosuppressants and immunomodulators. In general, the therapeutic efficacy of these drugs is rather poor, given the high frequency of relapses upon discontinuation of the drug. On the other hand, systemic (see: Remicade) or local immunomodulatory therapy with anti-TNFα, seems to induce a rapid and stable healing of the fistulas that complicate Crohn's disease, in a good percentage of patients.
The scarce tendency to definitive regression, whether spontaneous or drug-induced, of anal fistulas prompts the doctor to subject the patient to a delicate surgery. The surgical removal strategies of the fistula are numerous and varied: it will therefore be up to the doctor to determine how to act, based on the structure and length of the fistula. The ultimate goal of these interventions is the permanent eradication of the suppurative process without compromising the patient's anal continence
In-depth study: main types of intervention
Invasive interventions
- Fistulotomy: is typically reserved for patients with simple fistulas; this intervention consists in the literal flattening of the canaliculus. The procedure is not burdened with a significant risk of incontinence.
- Fistulectomy: involves the dissection of the entire fistula and a micro portion of the surrounding healthy tissue.
- Seton: it is a sort of large thread (tube) inserted through the fistula and subsequently joined at its two ends outside the body. The seton has two potential advantages: the first is the continuous drainage of the material contained in the fistulous tunnel ( such as pus), which escapes to the outside, preventing the development of complications and making subsequent surgical operations easier; the second advantage concerns the possibility of periodically putting the elastic in traction to slowly dissect the muscle tissue (ELASTODIERESIS or SLOW SECTION), cutting a new segment as the previous lesion heals; by doing so, clean cuts are avoided and the risk of incontinence.
- Two stage fistulectomy. As the term itself suggests, this operation is performed at two different times in order to minimize the risk of complications, such as damage to the anal sphincter and fecal incontinence. It is indicated in the treatment of complex, transphinteric and suprasphinteric fistulas, which also involve the anal muscles. In the first phase it involves the positioning of a seton which is periodically put in traction to slowly dissect the muscle tissue (ELASTODIERESIS or SLOW SECTION). The treatment with seton lasts a few months and is obviously of little satisfaction for the patient. By putting tension on the seton, the fistulous orifice is lowered more and more, allowing a fistulotomy or fistulectomy as soon as the section of the muscular plane (previously performed by means of a seton) gives way to solid scarring.
- Endorectal flap: consists of the reconstruction of the mucosa, submucosa and occasionally the circular muscular tunic, obtained by applying a well vascularized flap of the rectal mucosa (taken from the overlying rectum) on the internal opening of the fistula (fistulous orifice). With this procedure, the probability of incontinence is 35%.
Innovative and minimally invasive treatments that eliminate post-surgery complications such as fecal incontinence (which occurs in about 10-30% of cases).
- Closure of the fistula with fibrin glue. The surgery has a modest cure rate, in the order of 20-60%. It involves the injection inside the fistulous tunnel, previously cleaned (debriding), of a soluble mixture in order to seal it, just like a glue would do. The advantages are linked to the mini-invasiveness of the intervention, which cancels many of the complications typical of traditional interventions (including incontinence) and ensures a more rapid return to normal activities. However, the risk of recurrence remains high, with a low success rate of definitive healing of anal fistulas.
- Closure of the fistula with medicated plugs, resistant to infections and inert (they do not generate reactions from a foreign body). These less invasive treatments than traditional surgical interventions are performed by inserting special "medicated anal plugs" into the fistula, which favor the generation of new tissue, and are then spontaneously reabsorbed by the body. Also in this case the post-surgery complications they are almost nil, including the risks of incontinence; the therapeutic success rate is good (40-80%) but there is still an important risk of relapse.
- LIFT technique (ligation of inter sphincteric fistula tract): innovative surgical procedure which is based on the secure closure of the internal fistulous orifice (through the inter-sphincteric space and not via the endorectal route) and on the concomitant removal of the infected cryptoglandular tissue (cause of the fistulas). It is a recent minimally invasive, safe, effective and inexpensive technique, with a good success rate and low risk of recurrence.
- VAAFT (Video Assisted Anal Fistula Treatment): uses advanced diagnostic tools (operative fistuloscope) that first of all allow you to have a direct view of the fistulous path from the inside, also highlighting any local complications. In addition to vision, this device allows you to clean and treat the fistula itself from the inside, following step by step the operating phases on the monitor; moreover, the operation involves the hermetic closure of the internal orifice of the fistula transanal, important to avoid the passage of fecal material in the fistula. The technique is particularly indicated for the treatment of complex perianal fistulas. By treating the fistula from the inside, the risk of causing damage to the sphincters is eliminated; also in this case, therefore, the risk of postoperative incontinence is eliminated.
Most of the time, the patient is operated on in day hospital, which means that he can return home the same day of the operation. For more complicated fistulas, however, the patient can be held in the hospital for two or more days.
Post intervention
After the surgery, the perception of a slight pain must be considered an absolutely normal condition. Even blood loss is, to some extent, a fairly common post-surgery risk. Following an operation for an anal fistula, the pain can be controlled by administering painkillers, the doses of which must always be determined by the doctor.
In addition, to minimize pain, the patient can perform gentle compresses of warm-warm water (sitz bath) on the intervention area. To facilitate evacuation, the doctor may prescribe laxatives or stool softening drugs.
The possible intake of antibiotics (subject to medical prescription) to be taken by mouth can prevent the onset of post-surgery infections.
The major risks associated with surgery for anal fistulas are:
- Infections
- Faecal incontinence
- Relapsing fistula
The desirable approach is to avoid case number 2 as much as possible; in other words, we try to safeguard sphincter continence by adopting (when possible) minimally invasive techniques, even if this is to the detriment of the (lower) success rate and the (higher) risk of relapse compared to traditional surgical techniques However, such an approach often entails higher health costs, a not insignificant problem if we consider the current socio-economic situations of the country.
Post-surgery risks can be partially prevented by paying particular attention to wound hygiene and respecting absolute rest: in this way, the wound is prevented from becoming infected and the anal fistula from recurring.