Watch the video
- Watch the video on youtube
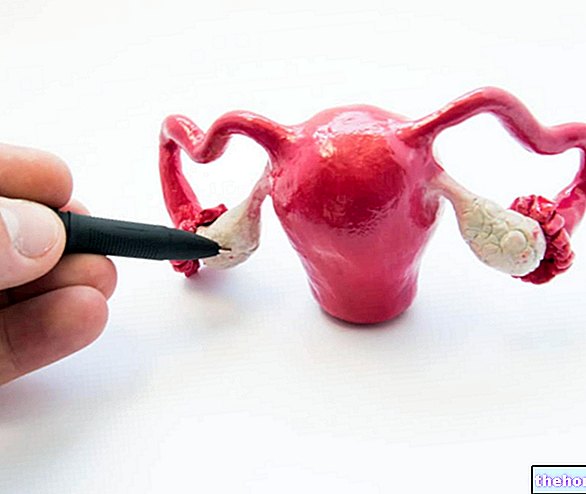
In uterine fibroid, the structure of the uterus is altered and fibrous cells are more abundant than muscle cells.
of the myometrium (hence "myoma"): medical statistics record an "incidence of cancer in 15-30% of women between the ages of 30 and 50, but it seems that the incidence rate is underestimated. In childbearing age, uterine cancer tends to expand, since this period coincides with the maximum estrogen secretion by the ovary. Not surprisingly, the birth control pill (estrogen-progestin therapy) could inhibit the onset - or growth - of uterine fibroid.After the age of 50, which for many women coincides with menopause, the fibroids in the uterus tend to regress or even disappear; the fibroid in the uterus of pregnant women, on the other hand, tends to expand, while remaining a benign form. If the contraceptive pill inhibited the growth of uterine fibroids, hormone-based replacement therapy during menopause could promote their development.

The uterine tubes and the cervix are two targets only rarely affected by fibroids; in fact, 95% of fibroids have the uterine body as their preferred locus.
Most uterine fibroids are asymptomatic, which means that women do not complain of symptoms of any kind (see article: uterine myoma, symptoms). In other cases, however, affected women may notice the tumor due to excessive intrauterine discharge (hypermenorrhea): menstruation is abundant and the cycle lasts longer. Given the abundant and prolonged blood loss, there is no lack of cases of anemia. A particular type of uterine fibroid, the pedunculated fibroid, involves pain caused by the twisted course of the tumor.
Another alarm bell is represented by the sensation of abdominal swelling associated with an abnormal heaviness localized to the lower abdomen; again, discomfort, constipation and pain on urination could be factors related to the manifestation of the fibroid in the uterus.
Pelvic ultrasound (external examination) is useful to clarify the location, volume and number of fibroids in the uterus; trans-vaginal ultrasound (performed using the vaginal probe) defines the morphology of the fibroid in a better way. This last technique is not recommended for large-caliber fibroids, since the probe cannot reach all the hidden areas of the "uterus" "from the fibroid.
Endoscopic techniques that visualize the interior of the uterus cavity are called hysteroscopies.
Magnetic resonance imaging represents "another diagnostic technique, the best in evaluating the possible involvement of the cells of the vaginal stroma and myometrium.
If the doctor assumes that the fibroid may also have resulted in the colon and rectum, the patient will undergo a rectosigmoidoscopy.
CT, on the other hand, is indicated to verify the possible invasion of neoplastic cells in the lymph nodes.
Based on the age of the woman, the type of fibroid, the histology, its location and the state of growth, the gynecologist chooses the most suitable therapy for the patient:
- Myomectomy: surgical removal of the uterine fibroid
- Hysterectomy: removal of the organ (preferable solution for women in menopause and for large fibroids, at an advanced stage)
- Embolization: involves blocking the blood supply in the uterus
- Pharmacological therapy (eg birth control pills) in women of childbearing age
The surgery can be performed in laparoscopy (traditional surgery which consists in "removing the tumor through an" opening in the abdomen); even hysteroscopy, already analyzed as a technique for detecting neoplasms, can be used for minor surgical interventions, aimed at completely eliminating the fibroid in the uterus.