Fifth part
CARDIOVASCULAR EFFECTS OF STAY AND TRAINING IN THE HIGHLAND
In addition to the strictly physiological aspects, concerning athletic performance, an interesting aspect for the sports cardiologist is that which concerns any cardiovascular effects of the stay and training at altitude. The regular practice of physical exercise reduces morbidity and mortality from cardiovascular diseases depending on the type, frequency, duration and intensity of physical activity, and it is reasonable to assume that the environmental conditions in which it usually takes place can play a significant role.

Wishing to summarize these concepts, we can say that hypoxia, however induced, is an effective erythropoietic stimulus, although the individual response appears variable. The haematological, muscular and respiratory adaptations that result from this stimulus allow the athlete to increase his ability to transport oxygen and use it in the suburbs. The ideal beneficiary of these practices is the endurance athlete, in which the increase in aerobic power follows the improvement in competition performance. On the other hand, the values of Hb and Hct reached are not very high, and in any case not such as to suggest a thrombotic risk. Physical activity at high altitude would seem capable of further reducing the risk of cardiovascular disease compared to physical exercise alone (but these data, extremely favorable to mountaineers and mountain tourism and unfavorable to us poor sailors, must be confirmed).
ALTITUDE PHYSIOLOGY
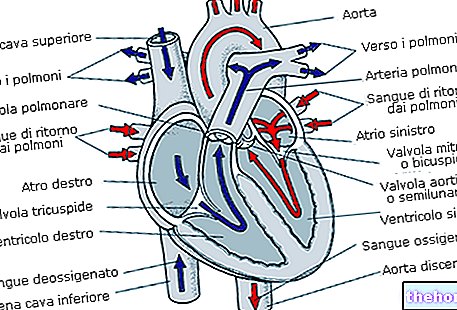
As the altitude increases, the air reaching the alveoli contains less oxygen. The partial pressures of carbon dioxide do not change much in absolute terms as this gas is only a small component of the air.
Since the Po2 alveolar decreases with altitude, the Pco2 arterial decreases in turn, resulting in a condition known as hypoxemia. With low levels of oxygen in the blood, less oxygen is available to the tissues, resulting in hypoxia (decrease of oxygen in the tissues). The degree of hypoxia depends on the altitude and how long the person has been there.
Hypoxemia initially gives rise to compensatory responses in an attempt to restore Po2arterial. If the Po2 drops below 60 mmHg, peripheral chemoreceptors are activated and the respiratory center increases ventilation. However, if ventilation increases too much with respect to metabolic demand, let Pco2 that the concentration of hydrogen ions in the blood will decrease, causing a decrease in the activation of both peripheral and central chemoreceptors and thus counteracting the effects of low oxygen concentration. respiratory alkalosis. With a decrease in blood acidity there is a shift to the left of the hemoglobin dissociation curve (increase in affinity). An increase in affinity means that less oxygen is released into the tissues, but it also means that more oxygen is bound to hemoglobin in the lungs.
If the stay at high altitudes lasts for a few days, the body begins to acclimate. The kidneys help maintain the acid-base balance by producing bicarbonate to compensate for the loss of hydrogen ions that accompanies the reduction of arterial PCo2. If the stay lasts a long time, other acclimatization phenomena intervene. In response to hypoxia, the kidneys secrete the erythropoietin hormone, which stimulates the synthesis of erythrocytes, resulting in an increase of up to 60% of the hematocrit, a condition indicated by the term polycythemia. The increase in the number of erythrocytes causes an increase in the concentration of hemoglobin in the blood, therefore an increase in the oxygen carrying capacity of the blood.
Upon exposure to low oxygen levels, oxyhemoglobin levels decrease, causing erythrocyte production of 2.3 DPG to increase. 2.3DPG decreases the affinity of hemoglobin for oxygen, increasing the release of oxygen to the tissues and counteracting the effects of alkalosis.
Sometimes, staying at high altitudes is not tolerated by the organism and the so-called can develop chronic altitude sickness. Initial symptoms include headache, dizziness, fatigue, and shortness of breath. This pathology can worsen to the point of causing disorientation and heart attacks. The symptoms of altitude sickness are mainly caused by hypoxia and polycythemia. Pulmonary vasoconstriction can also intervene, forcing the right side of the heart to work harder due to greater resistance.
Precautions and contraindications for altitude training
The heart patient may be at risk if exposed to high altitude due to the inability of the heart to adjust its performance in response to the stimulus generated by the reduced availability of oxygen. But from the experience reported by the various authors it can be affirmed that the operated heart patients can resume frequenting the mountains at altitudes below 3000 meters, as long as certain rules are respected. First of all, an accurate clinical evaluation is recommended that establishes, through specific instrumental tests the state of health of the patient, the functional conditions of his heart and the adequacy of the therapy. It is then advisable to limit physical activity during the first days of stay at high altitude during the acclimatization process; amount of effort and avoid physical activity in unfavorable weather conditions (very cold and windy or very hot and humid days); pay attention to any disturbances that may arise during exertion or immediately after (angina, dyspnoea, dizziness, excessive fatigue) ; do not do physical activity alone, not suspending the therapy in progress, avoiding the aspects of physical activity that involve a strong commitment no muscle and intense emotional stimulation. For lovers of alpine skiing it is advisable to avoid the rapid ascent to high altitude with the cable car and the rapid descent several times a day. It is better to give up a day in the mountains than to regret afterwards.
Before starting a period of training at altitude it is good to restore iron deposits, especially in those athletes with low blood values. In fact, Fe ++ deficient athletes are unable to increase red blood cells in response to altitude.
HYDRATION
Maintaining normal hydration at altitude is a very positive element for sporting performance at high altitudes: in fact it helps to eliminate the risks associated with dehydration without compromising the transport of oxygen to the tissues.
TRAINING AND LIFE AT ALTITUDE
Controlled studies on subjects who spent a long period at altitude living and training at moderate altitudes have never been able to demonstrate an effective improvement in performance at sea level. This method is instead valid if the training is carried out at high altitude.
DO NOT TAKE THE ATHLETE TO THE MOUNTAIN, BUT TAKE THE MOUNTAIN TO THE ATHLETE
In recent times, an alternative method has been developing, capable of providing a hypoxic stimulus "at home": the so-called hypoxic-hypobaric tents. These are closed structures in which the athlete stays for a few hours a day (usually at night), breathing air in which the partial pressure of oxygen has been artificially reduced. This method is certainly cheaper than the traditional one and easier to use. use, but there are currently considerable discussions on its lawfulness.
Short hypoxic exposures (1.5-2.0 hours) are sufficient to stimulate the release of EPO, therefore to increase the red blood cells.
LIVING AT HEIGHT AND TRAINING AT SEA LEVEL
This strategy combines acclimatization to a moderate altitude (2500m) with training at a lower altitude (1200m) and has been shown to improve performance at sea level for performance lasting 8-20 minutes.
TYPES OF EXPOSURE: 3 GROUPS
1. Lives at 2500m, trains at 1250m (High-Low)
2. Lives at 2500m, trains at 2500m (High-High)
Both groups living at 2500m show an increase in EPO, erythrocyte volume and Vo2max. Although VO2 max increased in both groups living at 2500m, only the group that did the low altitude training sessions he improved the time on 5000m by 1.5%.
3. Lives and trains at sea level on a similar type of terrain. (Low-Low)
High-Low subjects are able to maintain both training speed and peripheral oxygen flow during intense training sessions (= 1000m running at 110% speed compared to 5000m race speed) which are essential for performance of athletes who compete in running competitions.
High-High subjects during intense training sessions ran at lower speeds, with lower oxygen consumption, lower heart rate, and lower lactate peak.
While High-Low athletes are able to maintain the buffering capacity of muscles, this is not the case in High-High athletes.
Other articles on "Altitude Training"
- Erythropoietin and altitude training
- Altitude and training
- Altitude and altitude sickness
- Training in the mountains
- Altitude and alliance


.jpg)






















