Edited by Dr. De Domenico Giuseppe
vertebral
treatment
Hypercyphosis and hyperkyphotic attitude
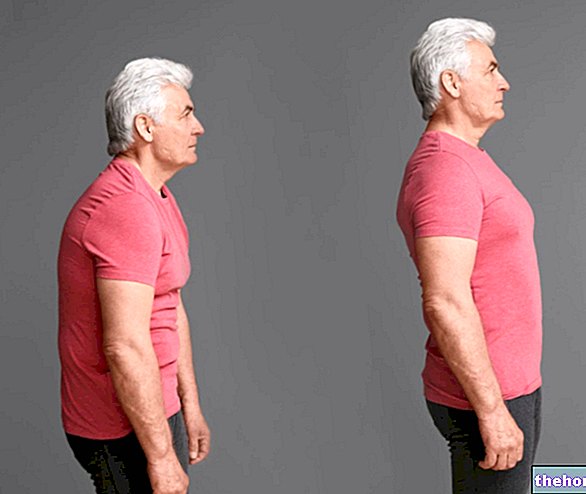
As mentioned above, the "Hypercyphosis, erroneously (but very commonly) referred to as "Kyphosis", represents an "accentuation of the normal dorsal curvature of the rachis.
We speak of pathological kyphosis or dorsal hyperkyphosis when the angle of the dorsal kyphosis is greater than 35 °. It is one of the most common situations, which can have psychological, postural, educational causes, and above all related to the profession. They are in fact a sedentary lifestyle. and the assumption of incorrect positions, especially in the office, to determine - in most cases - the accentuation of the physiological dorsal kyphotic curvature.
Classification
The medical classification includes postural kyphosis, congenital, idiopathic and osteochondrosis. Much more simply we distinguish:
1 - Mobile kyphosis, o hyperkyphotic attitude, when a voluntary straightening effort or a passive correction (e.g. dorsal decubitus), can easily be accomplished. There is no bone deformation and it is, in fact, a simple postural attitude. The treatment will only be kinesitherapic.
2 - Partially or totally fixed or rigid kyphosis, or Hypercyphosis, which can benefit from either a kinysitherapy treatment, or an orthopedic treatment or, in the most serious cases, surgery.
Hyperkyphosis, or the simple hyperkyphotic attitude, is often compensated for by lumbar hyperlordosis (kypholordosis) or cervical.
General analysis, evaluation and treatment of hyperkyphosis
It is possible, with due attention, to correct the attitudes of paramorphism by making use of the activity with weights, as long as it is aimed and acts for a preventive and ameliorative purpose. In fact, the goal will be to shape the muscles in order to minimize all the wrong postures of the spine.
At this point it becomes fundamental to quote the law of Borelli and Weber Fick: "The length of the fibers is proportional to the" shortening obtained by their contraction and this is approximately equal to half the length of the fibers ".
Generally speaking, there are four types of movement a muscle can perform:
- At full amplitude, maximum elongation maximum contraction
- Complete elongation, incomplete contraction
- Incomplete elongation, complete contraction
- Incomplete elongation and contraction
With the passage of time and with the repetition of the movements, it will therefore be possible to make morphological modifications of the muscle. Since the latter is essentially formed by a contractile part and a tendon, the effects deriving from the different movements will be the following:
in the first case the contractile part will increase and the tendon part will decrease with the result that the muscle will keep its length at rest but will increase its speed
in the second case the tendon part will increase more than the contractile part decreases with the result of a longer but slower resting muscle
in the third and fourth cases the result will be the same, the muscle at rest will be shorter.
In the case in question, hyperkyphosis, the persistence of an abnormal curve of the spine in the back region, in fact, first causes a lengthening of the dorsal muscles and a shortening of the pectoral one; in the long run it determines a progressive adaptation and consequent irrigation of the ligaments and a wedge deformation of the vertebral bodies.
This is Delphech's law: where the action of the load is greater, the growth of the vertebra slows down; where, on the other hand, the load is less, the growth is faster.
If the subject does not react in time, the load therefore presses on the concavity of the curve and the deformation gradually becomes irreversible.
An action therapy therefore assumes considerable importance immediate and targeted in order to block the evolution, therefore the increase in the severity of the paramorphism (risking to make it become a dysmorphism), and, indeed, improving and if possible completely correcting the alteration.
The sooner you intervene, the more likely you are to avert the danger, and the longer you persist with corrective exercises, the safer the positive outcome of the treatment.
Assessment
The value in degrees of the wedge deformation of each vertebral body is calculated by drawing two lines parallel to the vertebral plates on the X-ray plate and measuring the angle they form between them. The same is true if you want to know the global angle of a curve, that is, the angle formed by the tangents passing through the extremes of the curve: in this case, however, the extension of the two parallels would end out of the radiographic plates normally in use; it is therefore customary to derive it from the "crossing of the two perpendiculars to the two lines parallel to the bodies vertebral and more or less convergent depending on the value of the curve.
Action and evaluation of the treatment
Once the degree of deformity has been assessed, action is taken.
Hyperkyphotic pathology foresees, as already mentioned previously, a condition of hypertonicity of particular muscles; in particular of the muscles of the Great Dorsal, Great Pectoral, Anterior Deltoid, but also Great Teresus and Subscapularis; all muscles with a predominantly intra-rotatory action of the humerus and in part stabilizers of the scapulo-humeral joint.
To intervene on this type of pathology it is therefore necessary to intervene both on the muscles capable of carrying out a humeral internal rotation mentioned above, but also on those external rotators of the humerus And adductors of the shoulder blades.
It is therefore necessary boost up the Sottospinato, the Teres minor, the posterior deltoid and the trapezius; that is, all those muscles which perform an external rotation of the humerus and whose shortening can decrease the hyperkyphosis or the hypercyphotic attitude.
On the contrary, it will be necessary, instead, stretch and detension the great pectoral, the great dorsal, the great rotunda and the subscapular; all those muscles which perform an internal humeral rotation and which can consequently accentuate the hyperkyphotic curve.
The elongation of these muscles can be achieved through stretching exercises and, in less serious pathologies, with the use of overloads, however, in the light of the law of Borelli and Weber Fick, and exactly in the manner of "complete elongation and incomplete contraction';
By acting in this way, the resting muscle will be longer.
CONTINUE: Dorsal hypercyphosis "