The term dyschezia identifies a form of primitive constipation, in which the expulsion of faeces is difficult due to a functional or morphological alteration of the rectum. In the absence of other disorders, therefore, the motility of the upper tracts of the colon is normal and the transit of faeces is slowed down only at the rectal level.

Dischezia from functional causes
In the absence of anatomical alterations or underlying diseases, dyschezia is often the consequence of an incorrect lifestyle. In particular, the weakness of the abdominal muscles and pelvic floor - a consequence of sedentary lifestyle, aggravated by pregnancy and aging - compromises the efficiency of the abdominal press even during defecation. If this is associated with the habit of postponing defecation, the accumulation of feces in the rectal ampulla gradually tends to exhaust it, making it less sensitive to stimuli that originate from the relaxed state of its wall. Consequently, quantities of feces are always needed. greater to stretch the ampoule and give rise to the urge to defecate.
Among the muscles whose weakness or lack of coordination can cause dyschezia is the pubo-rectal muscle, involved in the so-called pubo-rectal syndrome. If this muscle contracts during defecation instead of relaxing, there is a "sharpening of the right-anal angle" which triggers the problems of obstructed defecation.
Dischezia due to pathological or iatrogenic causes
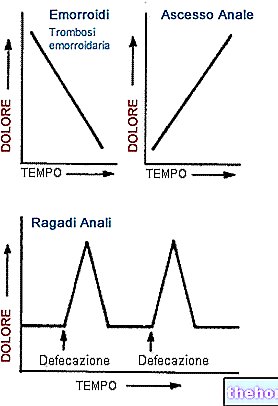
Dyschezia can also depend on painful affections of the anus (fissures, anism), which lead the patient to postpone defecation due to the pain it evokes.
Other causes of dyschezia include endometriosis, rectocele, rectal prolapse, cystocele, colpocele (in women) and Parkinson's disease.
Chronic laxative abuse can promote the atony of the muscles involved in defecation.
Associated symptoms
In the presence of dyschezia, defecation is painful and there is the perception of a foreign body in the rectum.
The voluntary inhibition of defecation, caused by pain, feeds a vicious circle, in which the patient may lose the natural ability to contract some muscles and release others (pelvic floor dyssynergy) during the defecatory act.
Complications
Chronic constipation traumatizes the rectal mucosa and can injure it, causing the so-called solitary rectal ulcer. The wound can cause rectal bleeding and mucorrhea, or the loss of rectal blood and / or mucus from the anus.
The weakening of the muscles and ligaments that support the rectum in its natural position can lead to its prolapse, that is, its exit from the anus.
Diagnosis
Anorectal manometry
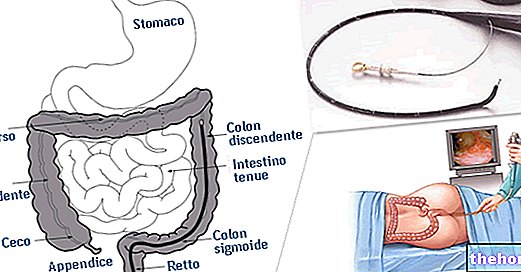
In the diagnosis of constipation due to obstructed defecation, the so-called anorectal manometry is particularly important. This examination consists in the introduction of a small sensor in the anal canal and in part of the ampulla, connected to a computerized system that records the pressures exerted on its walls.
With the collaboration of the patient, who must promptly satisfy medical requests, the anorectal manometry is therefore capable of evaluating the strength of the muscles involved in the continence of the rectal ampulla and of those responsible for the physiological evacuation of faeces. It also allows you to evaluate how the rectum responds to the evacuation stimulus. All this is possible thanks to the inflation and deflation of a balloon inserted into the rectum and connected to the probe.
Balloon ejection test
The doctor places a balloon in the patient's rectum, inflating it with 50cc of air. The distension of the rectal walls should trigger the urge to defecate and the expulsion of the balloon itself. If the subject is unable to expel the balloon, it means that there is a dysfunction of the pelvic floor.
DEFECOGRAPHY
See the dedicated article.
Treatment
In addition to the treatment of any underlying pathological causes, the so-called reeducation of alvus through biofedback or sphincter reeducation is important. It is a series of exercises to be performed under medical supervision and with the aid of computerized equipment, which help the subject to learn the mechanism of defecation in real time. The intervention aims to train the patient to contract certain muscles and to release others during the act of defecation. It is practiced in a similar way to manometry, then inserting a latex probe with a balloon at the end into the rectal ampoule.
The same aim is also pursued by electro-stimulation. It is a form of passive gymnastics, which induces the contraction of muscle fibers by means of a slight electric current applied by means of one or more electrodes inserted in the anal canal.
Definitely useful in case of dyschezia is the practice of regular physical activity of a general nature. The adoption of a varied diet, rich in water and soluble fiber, and the fact of following a certain time for the evacuation of the alvo can also be helpful.