So is the conjunctiva
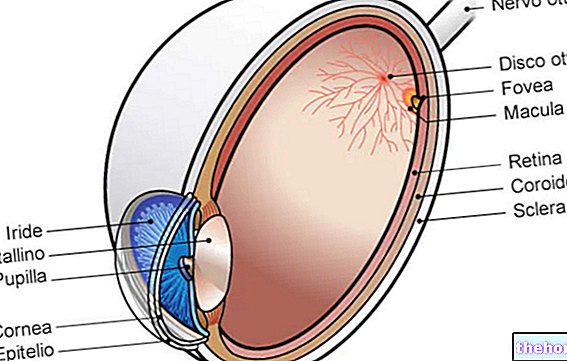
The conjunctiva is the thin mucous membrane that covers the anterior surface of the eyeball (except the cornea) and the inner surface of the eyelids.
Its main function is to protect the eye, thanks to the coating it provides, from foreign bodies and infections. Furthermore, this anatomical ocular structure helps to maintain the tear film and facilitates the sliding of the two opposite conjunctival surfaces, thus avoiding friction. in the blinking phases.
The conjunctiva can be the site of numerous pathological processes: inflammation (conjunctivitis), congenital malformations, benign or malignant neoplasms, dystrophic changes and degenerative diseases. Furthermore, general affections of the organism of various types have repercussions on the conjunctiva, such as infectious diseases, allergic reactions and metabolic disorders.

Structure
The conjunctiva is a mucous membrane, almost completely transparent, well vascularized and abundantly innervated by trigeminal filaments (called ciliary nerves).
From the histological point of view, the conjunctival tunic is made up of epithelial cells (columnar and squamous epithelium), arranged in 2-5 layers, and stroma (connective tissue). In addition, there is a glandular system, consisting mainly of goblet cells that contain mucin granules and provide for the production of the mucous layer of the tear film.
The conjunctiva can be divided into 3 anatomical parts:
- Eyelid (or tarsal) conjunctiva: made up of cylindrical epithelium, it is a thin, transparent, red or pink membrane. Following the skin, the conjunctival tunic begins at the free edge of the eyelids, then covers the posterior aspect of the tarsi, to which it adheres tightly.
- Bulbar (or scleral) conjunctiva: it is the part of the conjunctival tunic that is applied to the eyeball and covers the anterior surface of the sclera, with the exception of the corneal portion. Made up of a paving epithelium, the bulbar conjunctiva rests weakly on a lax connective lamina propria. The bulbar conjunctival tunic is smooth, very thin and so transparent that the white color of the sclerotic and the anterior conjunctival and ciliary vessels can be seen. In the medial position, then, the tarsal conjunctiva receives the upper and lower lacrimal dots, which represent the beginning of the lacrimal ducts.
- Conjunctiva of the fornixes: at the level of the space between the eyelids and the ocular globe, the conjunctival membrane folds and covers the upper and lower fornixes, allowing freedom to move the bulb.
Conjunctival sac
As a whole, the conjunctiva forms a kind of "pocket", which results from the folding of the bulbar membrane (which lines the eye) and of the eyelid membrane (adhering to the inner part of the eyelids). The conjunctival sac is closed when the free margins of the eyelids come into contact during blinking, while communicating with the outside when the eyelid fissure is open.
Lacrimal caruncle and semilunar fold of the conjunctiva
At the inner corner of the palpebral fissure, there are two formations that represent rudiments of embryonic structures: the lunate fold and the lacrimal caruncle.
The semilunar fold is a vertical fold of the bulbar conjunctiva, the free edge of which is concave. It extends from the upper to the lower fornix of the conjunctiva, but is visible only in its middle portion, being largely hidden by the eyelids.
The lacrimal caruncle is, on the other hand, a small rosy mucous outgrowth, rounded and raised, placed between the lacrimal portions of the eyelid margins; it contains a dense connective stroma, crossed by some bundles of smooth and striated muscle cells. The lacrimal caruncle has hair follicles with rudimentary hairs and attached sebaceous glands. It also contains accessory lacrimal glands.
Note: in humans, the lunate fold at the corner of the eye is considered a small vestigial remnant of the nictitating membrane, ie the "third eyelid" that is observed in other animals, such as birds and reptiles.
Functions
The conjunctiva has the main function of protecting the anterior surface of the eye.
Furthermore, it facilitates the sliding of the eyelids in the blinking phases and allows the eyeball to move, without friction at the level of its surfaces, thanks to the secretion of the mucin component of the tear film (a sort of viscous mucus that protects the cornea and allows the preeminent watery tears to stratify).
The conjunctiva contains, in fact, serous glands, muciparous (or goblet cells secreting mucus) and accessory lacrimal glands (of Krause and Ciaccio). These structures pour their secretion inside the conjunctival sac, thus helping to keep the ocular surface moist, clean and intact.
In addition to the physical and biological protection of tears, the conjunctiva has an immune defense system mediated by lymphatic elements, mostly located in the tarsal portion (lymphatic follicles). Due to its particular anatomy, in fact, the conjunctival tissue is particularly exposed to external agents, such as dust, pollen and bacteria.
Note: the conjunctival mucosa responds to stimuli of a different nature, which change its appearance. These reactions, for example, can give rise to a redness due to the dilation of the blood vessels of the conjunctiva (hyperemia) or cause a more serious picture with abundant discharge, pain, foreign body sensation and tearing, sometimes associated with edematous swelling (chemosis).
Conjunctivitis
Conjunctivitis is an "inflammation of the conjunctival surface. It is a frequent pathology, which can manifest itself in an acute or chronic form.
The causes can be various, but the most frequent are the following:
- Eye infections (due to bacteria, viruses, fungi or parasites);
- Seasonal or perennial allergies (hypersensitivity to pollen, cosmetics, dust mites or animal hair);
- Intense irritation from foreign bodies and chemical-physical agents (caused by drugs, heat, wind, dust and atmospheric pollutants, acids, alkalis, soap, cigarette smoke and fertilizers, excessive exposure to sunlight or other forms of radiation, etc. ).
Symptoms of conjunctivitis depend on the causes, but often include burning, itching, redness, photophobia, increased tear formation, swelling of the eyelids and a sense of foreign body (a feeling of having sand in the eye). In the infectious form, a catarrhal or mucopurulent discharge can be added to the listed manifestations (the eyes tend to "stick").
Therapy varies according to the type of conjunctivitis and is established by an ophthalmologist.
Bacterial forms can be cured with antibiotic eye drops therapy. In the case of allergic conjunctivitis, on the other hand, antihistamine and cortisone eye drops are used, which can be associated with the use of artificial tears and systemic antihistamine drugs.
Viral forms often caused by adenovirus and herpes virus have a longer and more difficult course than bacterial conjunctivitis. In general, frequent instillations of antibiotic eye drops are used (in order to prevent bacterial superinfection) and, with caution, topical cortisone drugs (to decrease hyperemia and conjunctival edema).
Subconjunctival hemorrhage
Subconjunctival hemorrhage appears as a bright red spot, not associated with other signs of inflammation. These blood extravasations below the conjunctiva result from a rupture of a capillary wall and usually appear following minor trauma , coughing and sneezing (for example, in the course of affections of the upper respiratory tract). In some cases, subconjunctival hemorrhage can be accompanied by systemic arterial hypertension, blood dyscrasias and viral conjunctivitis.
The disorder tends to resolve spontaneously in about 15 days, therefore no type of treatment is required. In any case, it is advisable to contact your ophthalmologist for an assessment.
Conjunctival foreign body
The presence of a foreign body at the conjunctival level causes unilateral symptoms, characterized by pain, difficulty in keeping the eye open, conjunctival hyperaemia, lacrimation and photophobia.
If held at the tarsal level, foreign bodies can cause corneal lesions due to the continuous rubbing of the eyelid during blinking. For this reason, they must be removed as soon as possible.
Conjunctival degenerations
Pinguecula and pterygium are benign degenerations of the conjunctiva, which appear as growths adjacent to the cornea. Both of these injuries cause redness, irritation, foreign body sensation and burning.
Pinguecula
The pinguecula is an accumulation of degenerated collagen, localized in the nasal and temporal conjunctival sector.

The pinguecula can represent the result of an inflammation of the ocular surface following trauma, caustic burns and peripheral corneal ulcerations.
Pterygium
Pterygium is a small, triangle-shaped fibrovascular formation caused by abnormal growth of the bulbar conjunctiva. This lesion progressively extends towards the cornea, until it covers it. Unlike the pinguecula, in fact, the pterygium has its own vessels.
This lesion typically occurs on the nasal side of the cornea and often results in a reduction in visual acuity by induction of astigmatism. In fact, the pterygium can distort the corneal surface, changing the refractive power of the eye.
The reduction of vision determines the need to remove the lesion surgically, even if recurrences are very frequent.
The causes behind the pterygium are still partly unknown, however chronic exposure to irritative factors (in particular, to the sun and wind) increases the risk of developing the disease.
Cicatricial pemphigoid
Cicatricial pemphigoid is an alteration characterized by progressive scarring and bilateral narrowing of the conjunctiva. This process is also associated with the simultaneous neovascularization, opacification and keratinization of the cornea.
The mechanism behind cicatricial pemphigoid is autoimmune.
At the beginning, the disease manifests itself in a similar way to a chronic conjunctivitis, causing hyperemia, discomfort, itching and secretion. The progression of the disease leads, however, to phenomena such as symblepharon (adhesion between tarsal and bulbar conjunctiva), trichiasis (introflexion of the cilia), keratoconjunctivitis sicca, and conjunctival keratinization.Chronic corneal lesions can lead to secondary bacterial ulceration and blindness.
The diagnosis can be confirmed by a biopsy. Treatment may require "systemic immunosuppression with dapsone or cyclophosphamide.
Tumors of the conjunctiva
The conjunctiva can be the site of benign or malignant neoplastic processes. In most cases, these originate from the epithelium (the most superficial layer of cells) or from melanocytes (present in the conjunctival epithelium).
Corneo-conjunctival intraepithelial neoplasia
Corneo-conjunctival intraepithelial neoplasia is the most common ocular surface tumor. It manifests itself with clinical pictures ranging from mild dysplasia to locally invasive carcinoma (rarely causes metastasis). Typically, it presents as a thickening or whitish, translucent or gelatinous conjunctival mass, often vascularized.
Therapy involves extensive surgical excision, sometimes associated with cryotherapy and reconstruction of the conjunctival plane. The use of topical chemotherapy can also be considered.
Squamous cell carcinoma
The most common malignancy is squamous cell carcinoma. This can originate from scratch or derive from a previous phase in situ. The initial forms resemble a pterygium, while the poorly differentiated ones have a gelatinous and translucent appearance. Squamous cell carcinoma, on the other hand, assumes a vegetative appearance, occupies the interpalpebral fissure and tends to protrude outwards. A prompt and rapid surgical excision, associated with cryotherapy, radiotherapy and topical chemotherapy, is generally associated with a good prognosis.
Lymphoid tumors
Non-Hodgkin's lymphoma of the ocular adnexa is quite rare (it represents about 8% of all extra-nodal cases). Generally, these cancers involve the lymphoid tissue associated with the mucous membranes, ie the so-called MALT (acronym for "mucosa-associated lymphoid tissue ") and can occur with the appearance of eyelid swelling or visual changes of various kinds.
Conjunctival melanoma
In most cases, pigmented tumors are benign, but they must always be considered as possible carriers of malignancy (the evolution is similar to that which leads to the formation of cutaneous melanoma).
Conjunctival melanoma is a rare neoplasm (it accounts for about 2% of malignant eye tumors). It can originate from scratch or result from the transformation of benign pigmented lesions (nevus and congenital melanosis) or pre-cancerous (primary acquired melanosis with atypia).
Conjunctival melanoma can cause metastases by lymphatic spread to the loco-regional lymph nodes and by blood. The therapeutic approach is guided by the size and location of the melanoma. In most cases, extensive surgical excision, often associated with cryotherapy, is the treatment of choice. In melanomas of large dimensions or located in unfavorable locations, radical surgery is indicated, which involves the removal of all the orbital contents.