an ergonomic approach
Edited by Dr. Giovanni Chetta
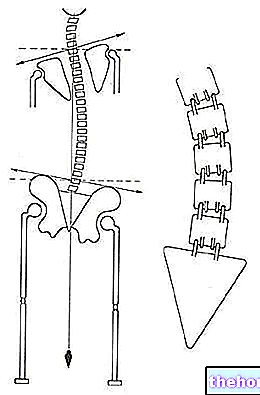
Almost always our adaptation to the flat ground associates the lumbar hyperlordosis with a rotation of the pelvis: from this arises, at the level of the rachis, the very common functional scoliosis which in severe cases causes, especially during growth and in old age, vertebral deformities (structural scoliosis). Scoliosis, in the majority of cases, however, remains the best possible attitude that the system of equilibrium, in a given subject, is able to obtain on a terrain that is not very congenial to him, such as the flat one. This explains the frequent failure of corrective braces. which, at the cost of great sacrifices by the wearer, once removed, usually cannot guarantee anything other than a very short period of realignment of the spinal column (the time sufficient for the postural system to realize that the most functional structure for that particular subject in that particular situation foresees a vertebral scoliosis).
In certain critical areas of the spine (the last lower cervical and lumbar vertebrae) the misalignment involves the creation of moments of force capable, over time, of causing real sliding forward or backward, listesis or spondylolisthesis, of a vertebra with respect to the adjacent one which, in the most serious cases, are accompanied by rupture, lysis, of a specific fragment, vertebral isthmus, of the slipped vertebra (spondylolysis).
The first consequence of spondylolisthesis is a strong, practically constant contraction of the muscles involved to prevent vertebral sliding in any way (muscles of the paravertebral showers); in this case there is no massage, stretching or joint mobilization that can solve this situation. The solution will be to permanently modify the postural attitude in order to cancel those moments of force acting on the vertebra whose result is a force that moves the vertebra from its original seat. After that it will be possible to intervene effectively with physiotherapy.
Misalignment, slipping and rotation of the vertebrae are the cause of the shrinkage, in addition to osteophytic degenerative processes due to overload, of the conjugation or intervertebral holewhich often occurs, in particular, in the lower areas of the lumbar and cervical tract, where the important brachial and sacral nerve plexuses are present, respectively. This narrowing, usually associated with strong contractures of the deep paravertebral muscles, is able to irritate the spinal nerve that crosses it which will project pain (neuropathies due to nerve root fibrosis), paresthesia, dysfunctions, etc., in the region of the body innervated by him. . This is often the real reason for the misdiagnosis (and therefore the failure of the related surgical interventions) of herniated discs, scapulohumeral periarthritis, epicondylitis, epithrocleitis, carpal tunnel syndrome.
In addition to simulating but often also being concomitant to these syndromes, the aforementioned mechanism is able to cause, for example, neck pain, brachialgia, back pain, back pain, low back pain, sciatica and further organic problems described in the next chapter.
Always at the level of the spine, misalignments, tensions and overloads represent a fertile ground for discopathies, protrusionied herniated discs, often affecting the intervertebral discs of the last cervical and lumbar vertebrae.
The tension and inflammatory processes deriving from the cervico-dorsal hinge manifest themselves in some cases as an accumulation of defined adipose tissue "hump of bison'.
Non-physiological tensions and postures of the girdle-humeral often lead, over time, into sub-acromial conflicts and pathologies affecting the rotator cuff.
The malposition of the pelvis leads, as a consequence, to anomalous rotations of the femoral necks. This will create tension in the coxofemoral joint at the level of the joint capsule, ligaments, tendons of the affected muscles with possible consequences such as coxalgia And groin pain (for inflammation of the inguinal ligament) in addition to early joint arthrosis (coxarthrosis) due to weight imbalance. Furthermore, an asymmetry at the level of the pelvis (one hemibacin more antiverse or retroverted than the other) is able to simulate a false leg length discrepancy.


During locomotion, when the lower limb, in the monopodalic phase, bears the weight of the body, the coxofemoral joint transmits the stress to the neck of the femur which acts as cantilever beam, anchored at one end to the femoral shaft (support structure) and subjected, at the other end, to the weight of the body. lever of about 3 times) and the moment of the resulting weight force causes the abductor muscles to exert a force 3 times greater than that of the body weight to keep the pelvis horizontal; the weight that acts on the coxofemoral joint, from the supporting side, is therefore about 4 times the weight of the body.
Thanks to their course parallel to the femoral neck, when the pelvis is in the correct position, the abductors, in particular the gluteus minor and medial muscles, by contracting, push the femoral neck longitudinally into the acetabular cavity. This compression is superimposed on the bending thrust of the femoral neck due to the weight force. In physiological conditions, a stress gradient is created on the femoral neck in which the compression is minimal on the upper part and maximum on the lower part. For this reason, in fact, the base of the femur neck. human has a strong layer of compact bone that is very resistant to compression (less to bending), while the rest is formed by porous bone. The physiological action of the abductors therefore allows an apparently fragile bone (and it actually is fragile in regards to flexion) to cope with a large load.
Unfortunately, when the pelvis is not positioned correctly, the postural tonic system during the monopodalic stance only partially recruits the gluteus gluteus minus and medial muscles and is forced to act, in large part, with other muscles, the most significant of which are the short and tenacious piriformis muscle (which originates on the anterior surface of the sacrum, between S2 and S4, and inserts on the superior margin of the greater trochanter) and the long and ribbon-like tensor muscle of the fascia lata (which originates on the anterior superior iliac spine and of the external lip of the iliac crest and is inserted, through the ilio-tibial tract, on the lateral tibial lateral condyle).
This has various consequences. The most important is that the physiological compression of the femur is lacking, which would allow it to tolerate the flexion forces deriving from the weight of the body, exposing it to the risk of fracture over the years and the increase in osteoporosis.
Secondly, the overstressing of the piriformis muscle favors the dreaded piriformis syndrome in which its structural alteration (increased volume and rigidity) irritates the sciatic nerve (which, depending on the case, passes inferiorly, superiorly or through the piriformis muscle) thus radiating pain and paraesthesia in the gluteal area and the lower limb (sciatica) sometimes leading to a misdiagnosis of lumbar disc herniation.
Finally, there is an aesthetic-physiological negative reflection, that is not very firm buttocks And cellulite. It is well known that, in this regard, diets, creams, pharmacological therapies (eg mesotherapy) etc. can do very little and in any case are not able to provide lasting improvements. their extreme thinness, accumulations of fat and cellulite on the thighs. The reason for this is that in reality it is a mostly postural problem. In fact, the recruitment of the tensor muscle of the fascia lata in monopodalic support, for the reasons previously described, causes the organism, to support the increased energy expenditure of this thin and long muscle located on the lateral part of the thigh, to create around it a reserve warehouse of oxygen and additional energy: cellulite. Further contributions to the formation of cellulite will naturally also derive from other factors such as: poor circulation (which, as we will see in the next chapter, is often of postural origin), sedentary lifestyle, incorrect eating habits, stress, environmental pollution, genetic predisposition, etc. Thus, the consequences of incorrect posture can also be not very firm buttocks (due to lack of use of the gluteus small and medium muscles) and cellulite (due to excessive use of the tensor fascia lata muscle). The slimming of the thighs and hips and the firming of the gluteal and abdominal muscles, obtained after a postural re-education, only confirms that health and beauty go hand in hand.
Other articles on "Posture and Wellness - Functional Scoliosis"
- Posture and well-being - Incorrect Podalic Support
- Posture
- Posture and Wellness - Foot and Posture
- Posture and well-being - Importance of plantar support
- Posture and well-being - Organic dysfunctions of postural origin
- Posture and well-being - Postural examination and re-education
- Posture and well-being