Physiological conditions for compiling a motor program for the little ones.
Sedentary lifestyle and obesity are a very common problem among the children of our society. About 4% of all children in Europe suffer from obesity and 25-50% of these maintain excess weight even in adulthood. developing early pathological situations.

Their physical characteristics, on the other hand, are different from those of their parents and it is good, therefore, to analyze the physiological requirements before approaching them to a particular sport or a physical exercise program. We therefore propose, below, a series of evidences resulting from numerous scientific studies, with which we hope to be able to make coaches and technicians reflect on physical activity.
Cardiovascular system
Children, being smaller than adults, also have small internal organs, including the heart. The Systolic Range is therefore also decreased, ie the quantity of blood expelled with 1 single beat (about 70 ml for the adult).
To compensate for the lower systolic output, the heart maintains a faster beat and a higher Maximum Heart Rate (HRM). In fact, unlike the 195-200 beats / min of a 20-year-old, a child can even reach an HRM of 215 beats / min. (Sharp, 1995). However, the Maximum Heart Rate remains constant throughout the pre-puberty years, so it does not seem to play any role in improving aerobic activity.
However, it should be borne in mind that, although the MHR is higher, the latter does not fully compensate for the lower systolic volume, demonstrable by the fact that the volume in l / min of arterial blood is lower when compared with adult individuals.
Unlike the latter, however, children receive a greater volume of arterial blood to the muscles during exercise, resulting from a greater difference in O2 concentration between arterial and venous blood (DAV - Artero-venous Difference). The calculated values of the DAV appear to be lower (between 12 and 20%) in pre-pubescent children than in pubertal children, although it is still uncertain whether the difference in O2 follows the same development as the child.
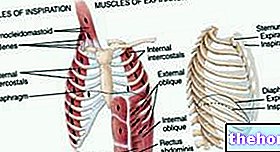
Respiratory system
During infancy the cardio-respiratory function begins its development and then ends when it matures. During this long journey, important changes in pulmonary function will be produced, with a progressive increase in ventilatory volumes at rest and during physical exercise.
The maximum ventilation values will go from 40-45 l / min at the age of 5-6 years up to 140-150 l / min in the adult male. Children also have a lower depth of breath and therefore need to an increase in the number of breaths.
Sharp found about 60 breaths / min in the child versus about 40 breaths / min in the adult. and Pneuma, air) which could worry parents and coaches, but which should instead be considered as a normal reaction of lively play activity.
Aerobic capacity
As a consequence of what happens with the organs most directly connected to this quality, such as the heart and lungs, aerobic capacity also increases with age. Studies on this (Krahenbuhl, Skinner, and Kort, 1985. and Bar-Or, 1983 ) report that the progression of improvement of this quality is quite similar for both males and females, with minimal variations throughout the pre-pubescent period, in which VO2max (maximum oxygen consumption) can report increases of the order of about 200 ml / min per year. It was also found that the VO2max of some children increased from 1.42 to 2.12 l / min over a period between the ages of 8 and 12 years, which is a 49% increase compared to baseline values (Bailey, Ross, Mirwald and Weese, 1978).
Obviously, there are also discrepancies in the two sexes, which become more marked in the pubertal period. Girls, in fact, reach a plateau of the peak of improvement for aerobic capacity, around the age of 12-14, maintaining values that are about 15% lower than boys, who, on the other hand, improve up to the age of 17-18. years (Cerretelli, 1985). To tell the truth, in females, a first gradual decline in values is already appreciated after the age of 8. Girls of this age, in fact, have an average value of VO2max of 50 ml / kg / min which drops to almost 40 ml / kg / min at the age of 16.
These differences in the two sexes are often interpreted by means of variations in body composition, that is, caused by the "increase in the fat mass of girls, as a direct consequence of maturation (although, according to other authors, some socio-cultural factors could influence a decrease in motor activity in females). However, some research reports that if we connect the VO2max values with the muscle volume of the lower limbs, the differences tend to cancel out. This data is confirmed by some studies on the behavior of VO2max / Kg, (ratio between max O2 consumption and body weight), used as an index of work power.
Possibility of VO2max training in pre-pubescent subjects
Overall, research indicates that if children do aerobic training 3-5 times a week, with continuous activity of at least 20 minutes for 12 weeks, improvements in VO2max of 7 to 26% are possible. a child can expect about 10% improvement in VO2max after a cardiovascular training program.
Pre-pubescent children undergoing systematic training are able to improve their VO2max, but not as effectively as adults do after an aerobic endurance exercise program.
It has been seen, in any case, that workouts aimed at this purpose do not show any particular effect until after the age of 11-12, so much so as to suggest that aerobic capacity is trainable near the pubertal stage, especially of males.
Many dispute the value of aerobic training because the reported improvements in VO2max should not be linked to "training, but to a" refined mechanical-coordinative efficiency. During the pre-pubertal period there is actually a continuous and fast adjustment of motor coordination, mostly due to changes in body size.
Furthermore, precisely during infancy, the nerve fibers improve their myelinated lining (myelination) which allows a faster conduction of the nerve impulse, with a consequent increase in the transmission of sensory and motor information and a better economy of energy expenditure, which it will positively translate into physical fatigue and oxygen consumption.
Anaerobic metabolism
Running, jumping, throwing, in addition to being of fundamental importance for the maturation of the child's basic motor patterns, represent gestures that could make us understand a child's predilection for anaerobic activities. Some explain that this type of activity turns out to be more of a psychological behavior than a predilection for anaerobic activity. Moreover, when compared with the general context of children's activities, short-term efforts are probably more limited than you don't seem at first glance.

At the time, the conclusions suggested the existence of a potential relationship between anaerobic muscle metabolism and physical maturation, which however is not always confirmed today. In general, children have limited capacity for anaerobic glycolysis up to a "post-puberty age, as they have significantly lower activity of glycolytic enzymes.
Eriksson et al. indicated that 11-13 year olds have about half the PFK (PhosfoFruttoKinasi) enzyme than adults, with the consequence that children cannot produce much energy through anaerobic metabolism and have to rely much more on aerobic metabolism For this reason, children have a much higher activity of enzymes related to aerobic metabolism than adults which, consequently, also allows them a better oxidation of fats during aerobic activity. Some studies (Kaczor-Ziolkowski-Popinigis- Tarnopolsky and Macek, -Mackova) have confirmed that children have low activity of the LDH (Lactate Dehydrogenase) enzyme responsible for the metabolism of lactic acid.
In conclusion
As we have seen, the organs and metabolic systems of children present some substantial differences compared to those of adults. Although still incomplete today, research on anaerobic and aerobic metabolism has shown that these two systems are not two separate entities but, rather, two metabolic systems that often interact with each other, not only in adulthood but also during the years leading up to puberty. The scientific reality also seems to suggest that aerobic physical activity is the most suitable for the physical activity of pre-pubescent children.
There are no specific exercises to report, rather it is essential to propose exercises and games that stimulate, in addition to learning, the right energy substrates, always keeping in mind the anatomical-physiological peculiarities of children. Once the technician has become aware of these characteristics, he will have to provide for the creation of a rich and quality motor base, which favors complex and as varied technical learning as possible (in the form of multidisciplinarity) to stimulate an "optimal structuring of motor schemes.
It is therefore useless to seek early specializations in the pediatric age, especially when scientific evidence informs us that up to the age of 12-13 the ability to manage intense activities and complex motor gestures are decidedly limited.

Personal Fitness Trainer
www.stranieri-fitnesstrainer.it